Lung metastases from Colorectal Cancer: Is Multislice Computed Tomography Reliable, which Provides Lung Palpation?
* Berjon L;
Lopez Pedreira MR;
Munoz MF;
Garcia Yuste M;
Matilla JM;
-
* Berjon L: Thoracic Surgery Department, Hospital Universitario Marqués de Valdecilla, Cantabria, Spain
-
Lopez Pedreira MR: Radiology Department, Hospital Clínico Universitario, Valladolid, Spain
-
Munoz MF: Research Support Department, Hospital Clínico Universitario, Valladolid, Spain
-
Garcia Yuste M: Thoracic Surgery Department, Hospital Clínico Universitario, Valladolid, Spain
-
Matilla JM: Thoracic Surgery Department, Hospital Clínico Universitario, Valladolid, Spain
Abstract
Purpose: To analyze the factors influencing the diagnostic accuracy of multislice CT, adding the benefit of intraoperative lung palpation to obtain more extensive surgical resection.
Materials and methods: A retrospective study was conducted on 77 patients who underwent resection for colorectal lung metastases from 2010 to 2016, with at least 3 years of follow-up. All patients underwent preoperative 64-slice CT scans with 1.2 mm slice thickness and intraoperative lung palpation. Analysis of the sensitivity, specificity, positive and negative predictive value of the multislice CT. Correlation between the number of nodules by CT, resected, and diagnosed as metastases (Spearman Rho). Classification into three groups: Group 1 (Accurate): CT and pathology nodule counts matched. Group 2 (Underdiagnosed): CT detected fewer nodules than pathology. Group 3 (Overdiagnosed): CT detected more nodules than pathology. The factors evaluated included the number of nodules, their size, laterality, the interval between CT scan and surgery, disease-free interval, recurrence, disease-free survival, and overall survival. Univariate analysis (Pearson’s Chi-squared t, Kruskal-Wallis t). Recurrence and survival analysis (Kaplan-Meier t) Significance p < 0.05. IBM SPSS Statistics 27.0 and Epid at 4.2 programs.
Results: Sensitivity 90.97%, specificity 31.57%, positive predictive value 83.34%, negative predictive value 48%. Significant correlation between nodules seen by CT, resected, and diagnosed as metastases (p < 0.001). Accurate group: 52(68%) patients, underdiagnosed group:8(10%) patients, Overdiagnosed group: 17(22%) patients. Factors associated with CT accuracy for detection of lung nodules: Size (p < 0.001), number (p < 0.001), laterality (p = 0.001), and CT-to-surgery interval (p = 0.022). Prognostic evaluation by the three groups: Disease-free interval (p = 0.665); early recurrence < 24 months (p = 0.06); 3-year survival: 43% vs. 79% and 54% respectively; 5-year survival 0% vs. 52% and 30% respectively (p = 0.210).
Conclusion: Size (< 9 mm), multiple metastases, bilateral metastases, and higher CT-to-surgery interval are influencing factors in the lack of CT scan diagnostic accuracy. Also, lung palpation contributed to a more extensive resection aimed at complete oncologic clearance in 10% of patients.
Abbreviations
- T: Test
- VATS: Video-Assisted Thoracoscopic Surgery
- DFI: Disease-Free Interval
- DFS: Disease-Free Survival
Introduction
The incorporation of multislice helical Computed Tomography (CT) has significantly advanced in the detection of small pulmonary nodules. Since its introduction in 1992, multislice CT technology has evolved from two to 320 imaging slices [1], offering improved image resolution and a 20% to 40% increase in sensitivity compared to conventional CT, enabling the detection of nodules as small as 2 mm–3 mm in diameter [2].
However, multislice CT sensitivity is inversely related to nodule size. While sensitivity is almost 100% for nodules larger than 10 mm, 68% for nodules 6 mm–10 mm, and further declines to 50%–61% for nodules smaller than 6 mm [3]. Therefore, intraoperative lung palpation can complement CT imaging, aiding in the localization and resection of all lung metastases, particularly smaller nodules. A meta-analysis by Macherey et al. found that patients with multiple, small, or mesenchymal metastases benefit most from lung palpation [4]. However, the clinical involvement of these occult nodules in CT and their impact on patient survival remains unclear [5].
Conversely, the increased sensitivity of multislice CT can lead to a higher rate of false positives, potentially resulting in unnecessary lung resections, a critical consideration in patients with limited pulmonary reserve.
Consequently, this study aims to analyze the diagnostic accuracy of multislice CT and its influencing factors, with a particular focus on undetected pulmonary nodules identified via intraoperative lung palpation, which can make for more radical surgery, and assess unnecessary lung resections, all in patients with colorectal lung metastases.
Material and Methods
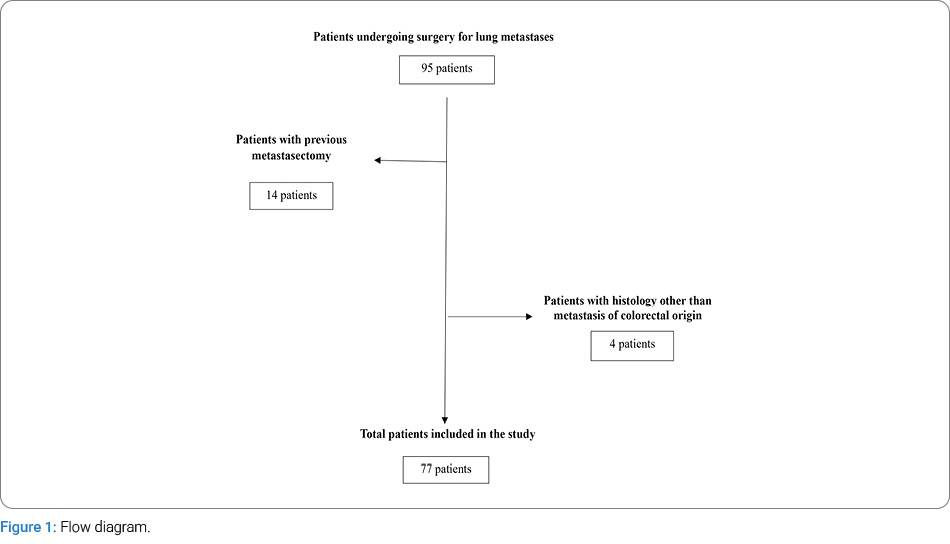
This retrospective study included patients who underwent surgical resection for colorectal lung metastases between January 2010 and December 2016 further follow-up until 2019. Inclusion criteria for surgery were controlled primary tumor and absence of extrathoracic disease, with the except for the presence of liver metastases. In cases of concurrent liver metastases, these were treated prior to addressing the lung disease. Staging was performed using a body CT scan and PET/CT scan in 59 patients. Suspected mediastinal lymphadenopathy was evaluated and ruled out by means of video mediastinoscopy. Fourteen patients with previous pulmonary metastasectomy were excluded for potential difficulty in palpation due to pleuropulmonary adhesions after the first intervention; four patients were excluded for having a non-colorectal histopathological diagnosis. A total of 77 patients who were treated by surgery during this period were included (Figure 1).
The 64 imaging-slice Revolution-Evo CT with a slice thickness of 1.2 mm and intravenous contrast was used for the preoperative imaging study.
The lung metastases were resected using an open or Video-Assisted Thoracoscopic Surgery (VATS) procedure. The open procedure involved anterolateral thoracotomy with costal and intercostal nerve preservation, a 7 cm–9 cm skin incision over the 4th or 5th intercostal space. The VATS procedure was biportal, via mini-thoracotomy in the 4th–5th intercostal space, with a 4 cm–5 cm skin incision and camera port over the 7th–8th intercostal space.
Lung palpation was performed in all patients included in the study. This technique involves tactile evaluation of the lung parenchyma during surgery. In the VATS procedure, digital palpation was performed by inserting a finger through the incision to explore the entire lung. In thoracotomy cases, manual palpation was carried out by inserting the surgeon’s hand to thoroughly examine the parenchyma. This intraoperative evaluation allows the detection of nodules not visible on CT imaging. The analysis consisted of evaluating the sensitivity, specificity, and positive and negative predictive values of the multislice CT. The correlation between the number of nodes seen by CT, those resected, and those diagnosed as colorectal metastases at microscopy of resected specimens was also studied using the Spearman Rho correlation test.
Finally, patients were classified into three groups based on the correlation between the number of nodules detected by CT scan and the number confirmed in the postoperative pathological evaluation:
- Group 1 (Accurate): The number of nodules detected by CT was similar to that confirmed pathologically.
- Group 2 (Underdiagnosed): The number of nodules detected by CT was lower than the number confirmed postoperatively.
- Group 3 (Overdiagnosed): The number of nodules detected by CT was higher than the number confirmed pathologically.
We aimed to identify the factors that could influence the CT accuracy for the detection of lung nodules and, therefore, predict which patients could benefit from intraoperative lung palpation to radicalize surgery, and which group was more likely to have unnecessary lung resections because of CT overdiagnoses. We evaluated the influence of the size (mm), which was measured by selecting the size of the largest metastasis, number of nodules (one or multiple), disease-free interval (months), which was the time from resection of the primary tumour to lung metastasectomy, and CT-to-lung-resection interval (days). We also analyzed the prognosis of the three groups, evaluating the survival times (months), recurrence, Disease-Free Interval (DFI), and Disease-Free Survival (DFS).
Pearson’s Chi-squared test was used to analyze the association of the qualitative variables, and Fisher’s exact test or the likelihood-ratio test were used for variables with more than two categories according to their suitability. Group comparisons were analyzed with the Student’s t-test for independent samples or the Mann-Whitney U test, depending on the case for two groups, and the one-way ANOVA or Kruskal-Wallis nonparametric test for more than two groups to compare. Finally, we also analyzed the clinical relevance of non-detected nodules using the Kaplan-Meier recurrence and survival analysis by subgroups. The data were processed using the IBM SPSS Statistics 27.0 for Windows program and the Epidat 4.2 program. Values of p < 0.05 were considered significant.
This study was conducted with informed consent from all patients and was approved by the Clinical Research Ethics Committee.
Results
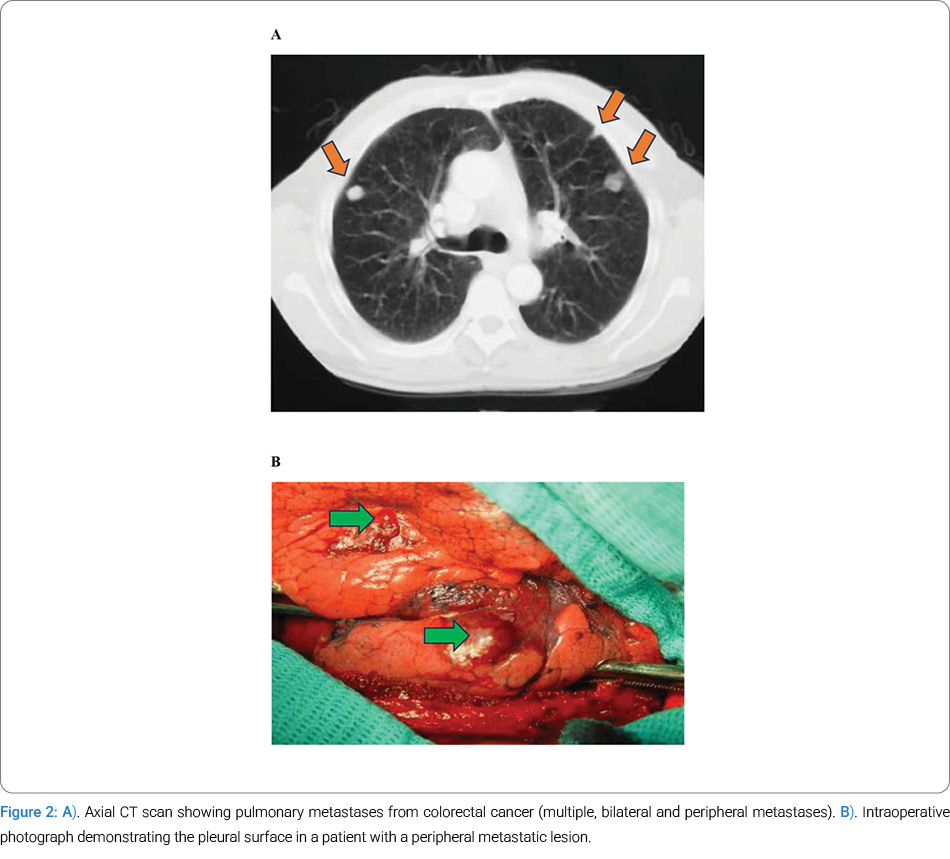
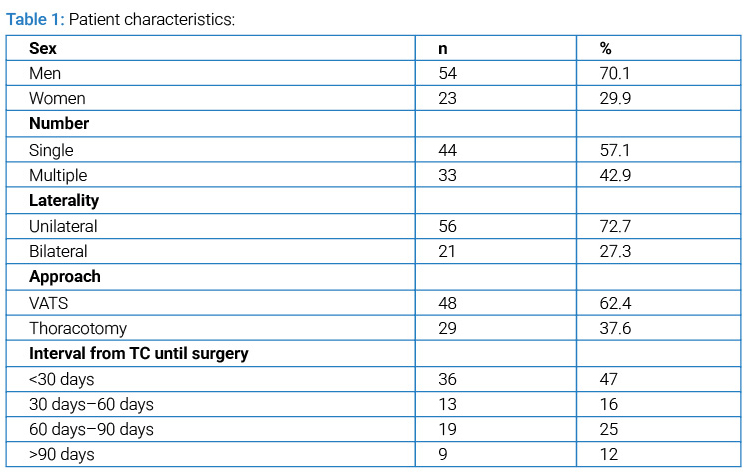
The sample comprised 77 patients, 54 (70.1%) men and 23 (29.9%) women. The mean age was 65.7 ± 10.6 years, and the patient demographic characteristics are set out in (Table 1) and (Figure 2). The mean number of nodules per patient was 2.03 ± 1.58 (range 1-8), and the mean size was 17.65 ± 9.03 mm (range 2–40). The main characteristics regarding nodule averages in CT, resected and analyzed, are set out in (Table 2).
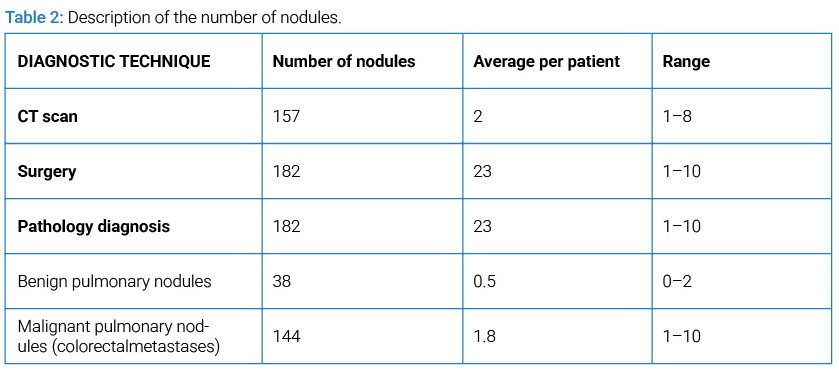
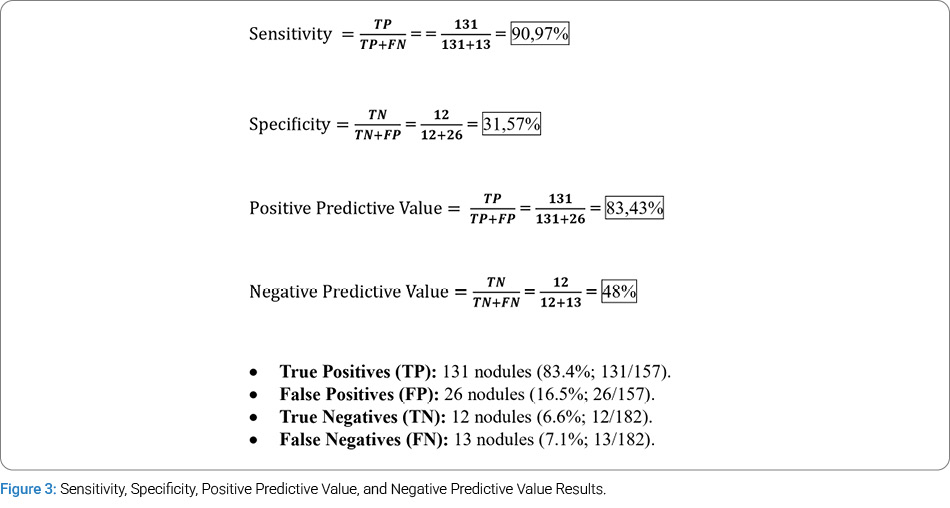
Our study identified a total of 38 (21%) benign nodules: 26 (14%) were false positives from the multislice CT, and 13 (7%) were false negatives that were detected through lung palpation. A total of 144 colorectal cancer metastatic nodules were also identified: 131 (83.4%) nodules were true positives from the multislice CT, while 13 (7,1%) nodules were false negatives on CT that were detected through lung palpation in a total of 8 (10%) patients. A sensitivity of 90.97% (CI 95% 85.94–96); specificity of 31.57% (CI 95% 15.48–47.65); positive predictive value of 83.43% (CI 95% 77.31–89.57), and negative predictive value of 48% (CI 95% 26.42-69.58) were obtained (Figure 3).
There was a statistically significant correlation between the number of nodules identified on CT and those resected (correlation coefficient = 0.76), as well as between CT-identified nodules and those confirmed as colorectal metastases on microscopic examination (correlation coefficient = 0.64) (p < 0.001).
Lung palpation in the 29 patients (37.6%) operated on with the thoracotomy procedure was manual. 48 patients (62.4%) were operated on with VATS, and in their case, lung palpation was digital.
Manual and digital lung palpation revealed nodules missed by preoperative CT imaging. Colorectal metastasis nodules were obtained using VATS in 4 patients (8.3%) and using thoracotomy in 4 patients (13.8%). Benign nodules were identified using VATS in 13 patients (27.2%) and using thoracotomy in 4 patients (13.8%). We therefore considered it important to also study this patient group in which unnecessary lung resections were performed.
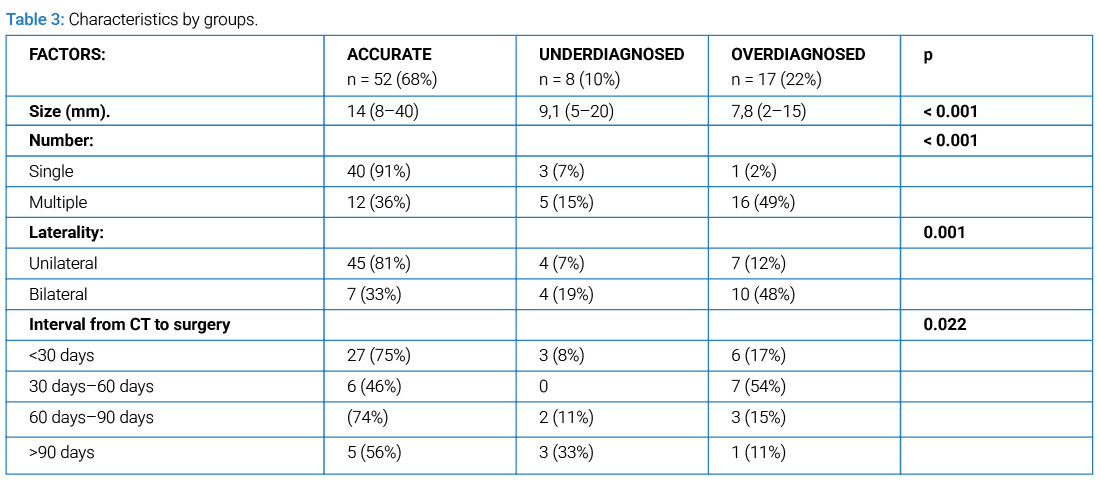
We divided the patients into three groups: 52 (68%) were correctly diagnosed, 8 (10%) were underdiagnosed, and 17 (22%) were overdiagnosed. CT accuracy for detection of lung nodules was significantly influenced by nodule size (p < 0.001), the number of metastases (p < 0.001), laterality (p = 0.001), and the interval between CT scan and surgery (p = 0.022), (Table 3).
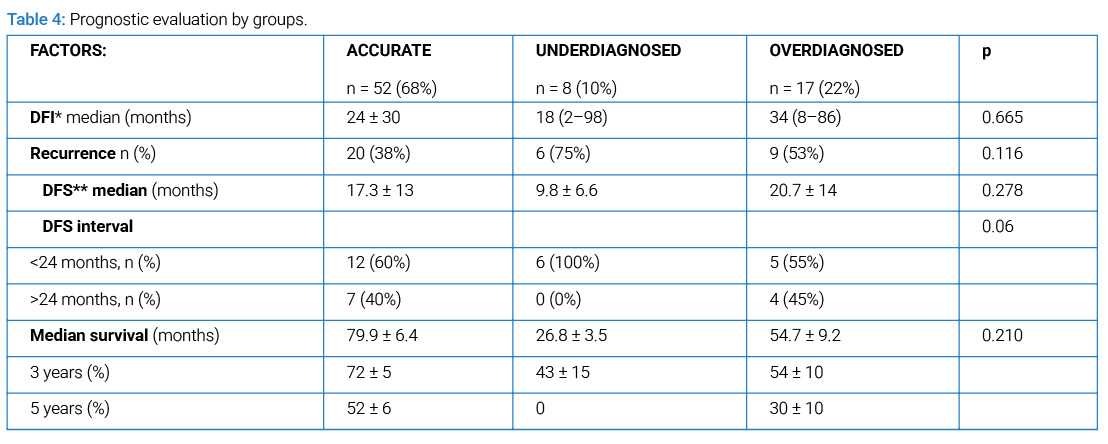
In relation to the prognosis of the underdiagnosed patients, where more malignant tumors than those shown by CT were resected, we found that half presented a DFI of less than 18 months. Furthermore, of the 8 patients in this subgroup, 6 relapsed, representing 75% of the underdiagnosed patients, and they all relapsed within 2 years (p = 0.06); average DFS in these patients was 9.8 months, less than the other two groups, although the difference was not statistically significant (p = 0.278). Average overall survival was 26.8 months, which was also less than the two comparison groups, although with no statistically significant differences (p = 0.210). Only 43% of the underdiagnosed patients were still alive after 3 years, and none survived to 5 years. Although no differences were found between subgroups (p = 0.210), overall survival was objectively lower in this patient subgroup (Table 4).
Discussion
While CT sensitivity for diagnosing malignant nodules can reach approximately 95% [6], the accuracy of modern helical multislice CT is influenced by several factors, including slice thickness. Pfannschmidt et al. reported sensitivities of 84% with 5 mm slices and 89% with slices thinner than 3 mm (p = 0.002) [7], demonstrating the impact of slice thickness on diagnostic performance. In this study, the patients were diagnosed using a 64 imaging-slice helical multislice CT with 1.2 mm thick slices. We obtained 91% sensitivity and an 83% positive predictive value; however, the negative predictive value fell to 48% and 16.5% false positives were obtained. Therefore, while reducing slice thickness increases both sensitivity and the rate of false positives, this trade-off must be carefully considered when planning surgical interventions.
Regardless of the current diagnostic progress, the debate around the need for careful exploration of the lung parenchyma to make surgery more radical continues. The present study aims to explore this issue in greater depth. A lung exploration was performed across all patients, using digital or manual palpation of the parenchyma. The correlation between the nodules identified by multislice CT, those resected, and those finally identified as metastatic was statistically significant (p < 0.001). We also observed a strong correlation between those identified by CT and those resected after applying the lung palpation technique (ρ = 0.76). Despite this good correlation between preoperative diagnosis and intraoperative findings, lung palpation identified colorectal metastases that had gone unnoticed in the CT in some 10% of patients. In 1 of every 10 patients, lung palpation effectively added radicality to the surgical process, identifying more metastatic nodules than those diagnosed preoperatively. In other studies, Chun et al. obtained 25% of nodules not detected by CT in patients with colorectal metastases [8], Cerfolio et al. obtained 20% of patients underdiagnosed by CT and found malignant nodules among patients with a higher likelihood of presenting occult nodules [5] and Zabaleta et al. obtained 12% occult nodules and a 9.5% probability of resecting more metastases in patients with one or two malignant nodules with respect to other histological subtypes [9].
A crucial consideration is the rate of false positives obtained by using more sensitive imaging and meticulous lung palpation, since this makes it possible to identify more nodules than those diagnosed. This combination of factors will inevitably contribute to identifying a higher proportion of nodules that are eventually found to be benign. Our study identified a total of 39 (21%) benign nodules: 26 (14%) were false positives from the multislice CT, and 13 (7%) were false positives from lung palpation. Therefore, lung resections should prioritize parenchyma preservation to minimize unnecessary lung tissue loss. Preoperative histological diagnosis can be a valuable tool in this regard, as Ludwig et al. recommend in their study [10].
Macherey et al. analyzed a total of 56 articles in their meta-analysis, which included 1,472 patients, and found 48.5% false positives. Indeed, more than one-third of all the nodules of primary-tumor patients were benign lesions [4]. Our study obtained 16,5% false positives, while Pfannschmidt et al. obtained 16% [7], Cerfolio et al. 13% [5], and Nakajima et al. 18% [11]. However, Zabaleta et al. and Nakas et al. obtained a smaller percentage of false positives, at 2.8% and 1.9% respectively [9,12]. The median size for the group of patients with occult nodules in the CT was 9 mm compared to 14 mm in correctly diagnosed patients. The Cerfolio et al. prospective analysis also found that patients with small nodules (1.6 cm vs. 2.3 cm) were more likely to be underdiagnosed by CT (p = 0.004) [5], and Kidner et al. also considered size a factor associated with underdiagnosis for nodules of 1.5 cm vs. 2.3 cm [13]. However, the overdiagnosed group presented significantly smaller tumor sizes.This suggests that smaller nodules detected by CT are more likely to be benign, and that nodule size is associated with lower diagnostic accuracy of the CT scan. Similarly, Nakajima et al. reported that nodules smaller than 5 mm in diameter detected by CT were often not lung metastases (p = 0.001) [11].
The number of nodules significantly impacted diagnostic accuracy (p < 0.001): with patients presenting multiple metastases being more likely to have CT underdiagnose their disease. This observation aligns with previous research. Zabaleta et al. reported statistically significant differences when comparing correct CT diagnosis in patients with a single lesion (86%) and those with multiple lesions (65%) (p < 0.001) [9], while Kinder et al. found that patients with an average of 2 nodules were more likely to present occult nodules (p = 0.001) [13]. In our work, we observed that almost half the patients with multiple metastases found by multislice CT were overdiagnosed, compared to the 91% of patients with single metastases who were correctly diagnosed. Therefore, patients with multiple metastases are more likely to have their disease underdiagnosed by CT. While lung palpation can identify nodules missed by CT, it is important to recognize that these patients will tend to be overdiagnosed by CT.
The laterality of the metastases was another factor of significant influence (p = 0.001). 80% of patients with unilateral metastases were correctly diagnosed, compared to the 48% with bilateral metastases who were overdiagnosed. These findings suggest that patients with bilateral nodules on CT are more likely to receive false positives, so prior histological diagnosis would be justified to prevent unnecessary lung resections, since this is a bilateral procedure with the added comorbidity this entails.
Finally, another factor that had a significant influence on CT accuracy for the detection of lung nodules was the time to surgery. The longer the time interval, the higher the proportion of underdiagnosed patients (p = 0.022). We found that up to 33% of patients with CT-to-surgery intervals of more than 3 months had nodules that would not have been detected if it had not been for lung palpation. These findings suggest that lung palpation is a useful and necessary tool for patients with long intervals from when the CT scan was done, and will contribute to more radical surgeries.
The clinical significance of occult nodules underdiagnosed by CT remains unclear. One possible explanation is the presence of micrometastases at the time of primary tumor diagnosis, which are not detectable by CT but may later become palpable as they grow. Does this imply a worse prognosis for these patients, or could it be more favorable due to the more radical surgery they undergo? The answer remains uncertain. In our experience, although we did not obtain statistically significant results, what we could see is that the DFI was shorter in the group of patients with underdiagnosed occult nodules than in the other two groups. The average was 18 months, compared to 24 months for the correctly diagnosed group and 34 months for the overdiagnosed group. Disease behavior was also worse in the underdiagnosed group, where, despite the absence of statistical significance, we found that 6 of the 8 patients had a recurrence, and all of them within 2 years. We also saw lower overall survival in this patient subgroup. Therefore, although we did not obtain statistically significant differences, we found that the underdiagnosed patient subgroup tended to have a worse prognosis. This raises the question regarding the most appropriate treatment procedure for these patients and whether they would benefit from systemic treatment.
Conclusions
In conclusion, despite the increased sensitivity of multislice CT and the strong correlation between the number of nodules detected on CT and the number resected, intraoperative lung palpation identified additional metastases in 1 of every 10 patients, adding radicality to the surgical process. We should pay special attention to patients with multiple and bilateral metastases and with small nodules, given the lack of CT accuracy for the detection of lung nodules as shown in this work, and those with CT-to-surgery intervals of over 3 months. While we hypothesized that patients with occult nodules identified via palpation might have a worse prognosis and earlier recurrence, this association could not be statistically confirmed in our study.
The limitations of this study presents are partly due to sample size, since it is a single-site study, and partly due to the retrospective nature of the design. Larger clinical trials with more scientific evidence would therefore be needed to reaffirm these conclusions.
Acknowledgments
I thank J. Berjon Rufes for his collaboration and special drive in the preparation of the manuscript.
References
- Calzado A, Geleijns J. Computed Tomography. Evolution, technical principles and applications; Tomografia computarizada. Evolucion, principios tecnicos y aplicaciones. Revista de fisica medica. 2010;11.
- Sluimer I, Schilham A, Prokop M, Van Ginneken B. Computer analysis of computed tomography scans of the lung: a survey. IEEE Trans Med Imaging. 2006;25(4):385–405.
- Collie DA, Wright AR, Williams JR, Hashemi-Malayeri B, Stevenson AJ, Turnbull CM. Comparison of spiral-acquisition computed tomography and conventional computed tomography in the assessment of pulmonary metastatic disease. Br J Radiol. 1994;67(797):436–444.
- Macherey S, Doerr F, Heldwein M, Hekmat K. Is manual palpation of the lung necessary in patients undergoing pulmonary metastasectomy?. Interact Cardiovasc Thorac Surg. 2015;22(3):351–359.
- Cerfolio RJ, McCarty T, Bryant AS. Non-imaged pulmonary nodules discovered during thoracotomy for metastasectomy by lung palpation. Eur J Cardiothorac Surg. 2009;35(5):786–791.
- Kang MC, Kang CH, Lee HJ, Goo JM, Kim YT, Kim JH. Accuracy of 16-channel multi-detector row chest computed tomography with thin sections in the detection of metastatic pulmonary nodules. Eur J Cardiothorac Surg. 2008;33(3):473–479.
- Pfannschmidt J, Bischoff M, Muley T, Kunz J, Zamecnik P, Schnabel PA, et al. Diagnosis of pulmonary metastases with helical CT: the effect of imaging techniques. Thorac Cardiovasc Surg. 2008;56(8):471–475.
- Chung CC, Hsieh CC, Lee HC, Wu MH, Huang MH, Hsu WH, et al. Accuracy of helical computed tomography in the detection of pulmonary colorectal metastases. J Thorac Cardiovasc Surg. 2011;141(5):1207–1212.
- Zabaleta J, Aguinagalde B, Izquierdo JM, Mendoza M, Basterrechea F, Martin-Arruti M, et al. Determination of a low risk group for having metastatic nodules not detected by computed tomography scan in lung metastases surgery. Arch Bronconeumol. 2013;49(12):518–522.
- Ludwig C, Cerinza J, Passlick B, Stoelben E. Comparison of the number of pre-, intra- and postoperative lung metastases. Eur J Cardiothorac Surg. 2008;33(3):470–472.
- Nakajima T, Yasufuku K, Iyoda A, Yoshida S, Suzuki M, Sekine Y, et al. The evaluation of lymph node metastasis by endobronchial ultrasound-guided transbronchial needle aspiration: crucial for selection of surgical candidates with metastatic lung tumors. J Thorac Cardiovasc Surg. 2007;134(6):1485–1490.
- Nakas A, Klimatsidas MN, Entwisle J, Martin-Ucar AE, Waller DA. Video-assisted versus open pulmonary metastasectomy: the surgeon’s finger or the radiologist’s eye? Eur J Cardiothorac Surg. 2009;36(3):469–474.
- Kidner TB, Yoon J, Faries MB, Morton DL. Preoperative imaging of pulmonary metastases in patients with melanoma: implications for minimally invasive techniques. Arch Surg. 2012;147(9):871–874.
- Krishnan K, Khanna C, Helman LJ. The molecular biology of pulmonary metastasis. Thorac Surg Clin. 2006;16(2):115–124.
Cite this article
Berjon L, Lopez Pedreira MR, Munoz MF, Garcia Yuste M, Matilla JM. Lung metastases from colorectal cancer: is multislice computed tomography reliable, which provides lung palpation?. Clin Oncol J. 2025;7(2):1–7.
Keywords
Lung metastasectomy; Lung palpation; Colorectal metastases; Colon cancer; Lung metastases; Metastasectomy procedure
Copyright
© 2026 Berjon L. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
