Abstract
Infectious exacerbations in COPD are the most frequent cause of exacerbations, up to 70%. For patients with advanced COPD with multiple hospitalizations for infectious exacerbations, it is appropriate to pursue a microbiological diagnosis. If clinical or radiological recovery is not complete, it is necessary to extend the diagnostic spectrum with chest TAC and bronchoscopy to rule out noninfectious causes or infectious complications. We are presenting a case of a patient with advanced COPD and multiple exacerbations, figuring out postobstructive recurrent pneumonia in the Right Lower Lobe (RLL) and squamous cell lung carcinoma in the Left Upper Lobe (LUL).
Introduction
An exacerbation of COPD is an event characterized by increased of dyspnea, cough, and sputum production [1]. In the initial evaluation, a chest radiography is needed to exclude pneumonia, laboratory studies, an electrocardiogram, and arterial blood gas [4]. Sputum culture may be helpful in patients who have frequent exacerbations of COPD or fail to respond to initial antibiotic therapy [2]. In case of recurrent pneumonia in the same lung lobe should be evaluated to rule out anatomic abnormality with TAC and bronchoscopy [3,5,6].
Case Presentation
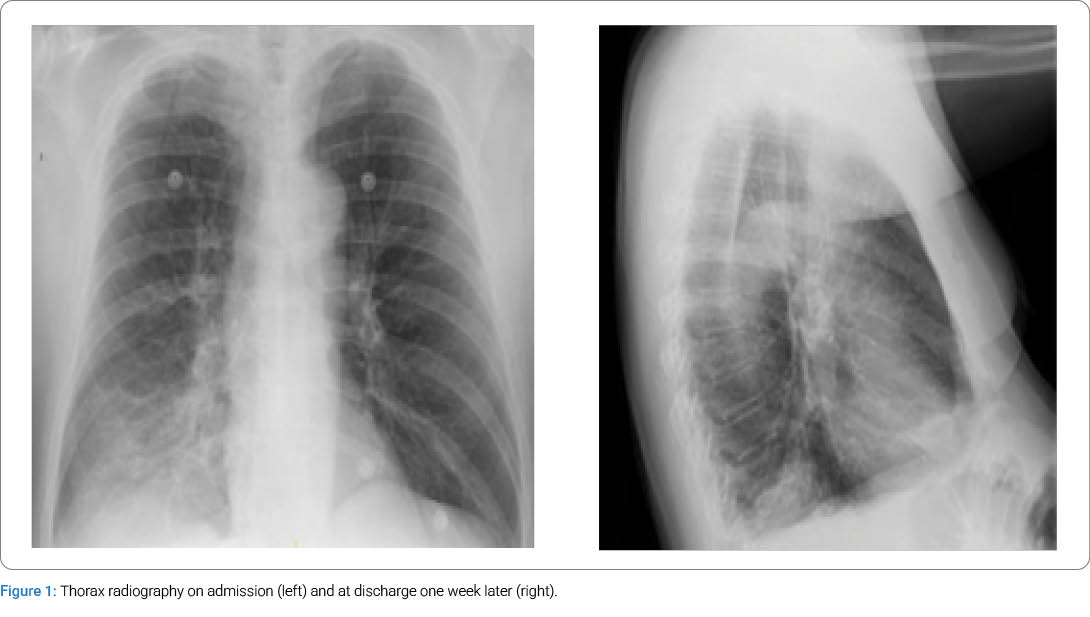
63-year-old male with medical history of: hypertension, obese with BMI 31, chronic rhoncopathy, ruling out sleep apnea on two occasions, COPD GOLD E4 (according to the latest GOLD guidelines of 2024, [7] with very severe airflow obstruction, baseline dyspnoea 2 mMRC–3 mMRC, former tobacco and hashish user, with a pack-year index of 40, chronic respiratory failure and long-term oxygen therapy carrier. He requires seven hospital admissions for infectious exacerbations and exacerbated chronic respiratory failure since 2018, of which in 2018, Streptococcus pneumoniae was positive in urine antigen, and in 2022, Stenotrophomonas maltophilia was sensitive to levofloxacin isolated in sputum. In the last admission, it is considered starting noninvasive mechanical ventilation, but the patient has always experienced clinical improvement and correction of the parameters of arterial blood gases on discharge after receiving medical standard treatment: short-acting bronchodilators, systemic glucocorticoids, and antibiotics. In April 2024, he was admitted for a right lower lobe pneumonia with good clinical evolution and resolution of the infiltrate in the subsequent chest X-ray, receiving empirical antibiotic therapy, glucocorticoids, and bronchodilators (Figure 1).
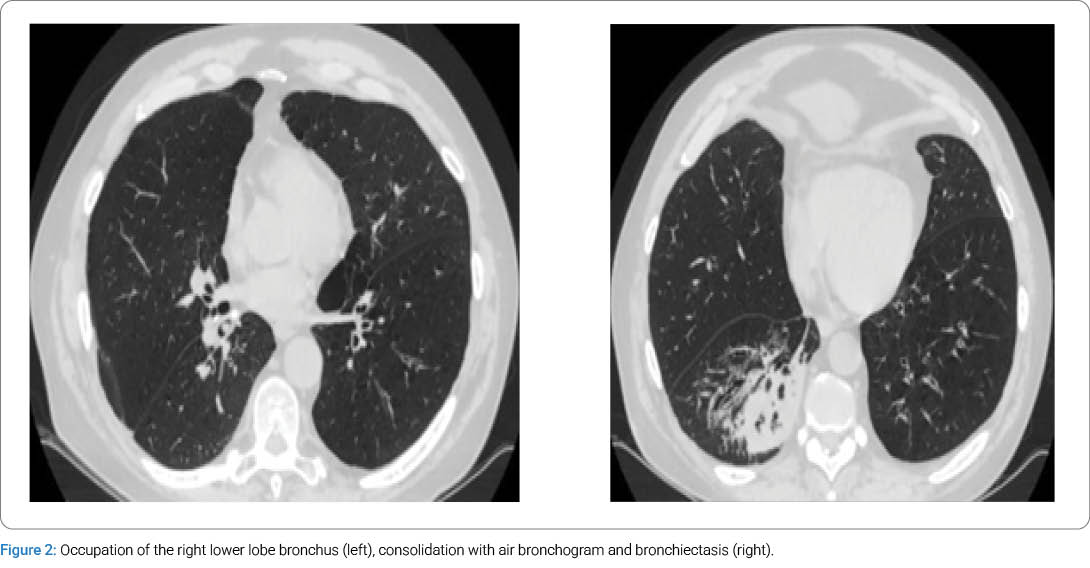
Given the multiple hospital admissions and the worsening of his functional class, the BODE index is calculated, and he meets 5 criteria, so the option of lung transplantation is taken into account. A chest CT scan performed on June 17, 2024 shows extensive paraseptal emphysema predominantly in the upper lobes, consolidation in the Right Lower Lobe (RLL), and bronchiectasis resulting in a discrete loss of volume. The radiologist comments that these findings could be related to an infectious process without being able to rule out other diagnostic possibilities, recommending a control CT in 4 weeks (Figure 2).
New admission in July 2024 for pneumonia in the RLL isolating SARS-CoV-2 virus and probable bacterial superinfection, receiving standard treatment with good evolution. Chest CT scan is repeated on July 25, 2024, describing radiological worsening of the airspace consolidation of the right lung base, with greater volume loss and air bronchogram. New admission in September 2024 for recurrent pneumonia in the RLL. This time, bronchoscopy is performed with findings of bronchitis and obstruction of the RLL bronchus by a foreign body that is completely extracted, and it is compatible with organic rest (Figure 3).

After its extraction, the mucosa of the RLL is visualized, and it is thickened, hindering the exit of the medial segment of the right lower lobe, but the other branches of the basal pyramid are correctly observed; biopsies of the mucosa of the RLL bronchus are taken. It is also noted thickening and irregularity of the mucosa of LUL, but with a permeable distal lumen, and biopsies of this area are also taken. After removal of the foreign body and establishing standard medical treatment, the patient improves and is discharged. The pathological anatomy of the bronchus of the RLL is compatible with chronic inflammation, that of the LUL bronchus is compatible with a squamous lung carcinoma T1bN0M0, being inoperable due to functional criteria, and the thoracic tumor committee decides on radiotherapy and follow-up by the palliative care unit.
Discussion
Respiratory infections are the main causes of exacerbation of COPD [1]. Pneumonia is more frequent in patients with COPD, and the resolution of radiological infiltrates may be slower due to the ineffectiveness of the cough, but in the case of repeated pneumonias in the same lung lobe or pneumonias with slow resolution, it is necessary to complete the study with CT and bronchoscopy to rule out the presence of an endobronchial lesion causing obstruction and postobstructive pneumonia [5]. In this case, there were two different lesions in the segmental bronchial branches at the same time: a foreign body causing distal obstruction in the RLL and a squamous endobronchial tumor in LUL, which meant that the patient with severe COPD could not be referred for lung transplantation.
Cite this article
Lucrezia G, Nyberg CP, Vargas NB, Abelende JMM, Tarbet CER, Manuel RG. Advanced chronic obstructive pulmonary disease with postobstructive recurrent pneumonia in right lower lobe and squamous cell lung carcinoma in left upper lobe. Clin Oncol J. 2026;7(2):1–3
Keywords
Chronic obstructive pulmonary disease (COPD); Infectious exacerbations; Postobstructive recurrent Pneumonia; Foreign body aspiration; Squamous cell lung carcinoma
Copyright
© 2026 Lucrezia Giannozzi. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
