Long Term Clinical Outcomes of Compartmental Clearance of Infratemporal Fossa in Very Advanced Subset of cT4b Carcinoma of Buccal Mucosa- Gingivo Buccal Complex
* Kalyani N;
* Katna R;
Maini A;
Chalke S;
Paatni P;
* Bhosale B;
* Patil V;
Karpe A;
-
* Kalyani N: Jaslok Hospital and Research Centre, Pedder Road, Mumbai, India
-
* Katna R: Jaslok Hospital and Research Centre, Pedder Road, Mumbai, India; Bombay Hospital and Research Centre, Marine Lines, Mumbai, India; Vedant Hospital, Thane, India
-
Maini A: Vedant Hospital, Thane, India
-
Chalke S: Vedant Hospital, Thane, India
-
Paatni P: Vedant Hospital, Thane, India
-
* Bhosale B: Jaslok Hospital and Research Centre, Pedder Road, Mumbai, India; Bombay Hospital and Research Centre, Marine Lines, Mumbai, India; Vedant Hospital, Thane, India
-
* Patil V: Vedant Hospital, Thane, India; P. D. Hinduja Hospital and research Centre, Mumbai, India
-
Karpe A: Vedant Hospital, Thane, India
Abstract
Aim: T4b carcinoma of Buccal Mucosa- Gingivo Buccal complex has poor outcomes. The analysis aims to evaluate long-term clinical outcomes following infratemporal fossa clearance for stage T4b carcinoma of the Buccal Mucosa-Gingivo Buccal complex.
Material and Methods: Ninety-three patients from the maintained data set of 1223 patients with oral cavity carcinoma were evaluated for the current retrospective analysis. All had T4b disease on imaging and underwent bite composite resection with ITF clearance.
Results: The median age of the cohort was 50 years. At the last follow-up, 55 patients were alive. 43 patients had loco-regional recurrence (ITF recurrence: 13), and 16 patients had distant metastasis.
At median follow-up of 53 months (95% CI: 36 months–69 months), the 5-year LRC, DFS, and OS was 46%, 44%, and 56%, respectively. On multivariate analysis, the presence of advanced nodal disease and pathological ITF involvement was found to be significant for overall survival.
Conclusion: ITF clearance is feasible in clinical practice and provides a long-term curative option for this group.
Introduction
Oral Squamous Cell Carcinoma (OSCC) comprises a diverse array of presentations due to distinct anatomical subsites, histopathological features, and risk factors. Infratemporal fossa, being a three-dimensional, complex space that inhabits vital structures, has become a topic of debate over the years. The anatomical complexity of the Infratemporal Fossa (ITF) and Masticator space makes it challenging to achieve an R0 resection [1]. Management of infratemporal fossa disease has been evolving over time, changing the standard of care.
In 2006 and 2007, after the publication of Liao et al., which showed positive trends toward surgical management for T4b tumors, surgeons began exploring the surgical domain for these previously labeled unresectable tumors [2,3]. Hence, it was established that although not all, a certain subset of T4b could be managed surgically with comparable outcomes to T4a OSCC.In 2020, we published the clinical outcomes of Compartmental Clearance of the Infratemporal Fossa in an advanced subset of T4b Carcinoma of the Buccal Mucosa/Alveolus [3]. Now, we present an update on the same with a larger cohort and long-term clinical outcomes.
Material and Methods
All patients with locally advanced carcinoma of the oral cavity (T4b – AJCC 8th edition) with clinical ITF involvement were included for the present analysis from well maintained prospective patient records. All patients underwent a thorough preoperative clinical examination supplemented with imaging (contrast-enhanced CT scan of face and neck) and distant metastasis workup for lung metastasis (CT scan of thorax or PET-CT). Patients with masticator space involvement with more than 2 of the following structures involved (on CT scan), i.e., medial and lateral pterygoid muscles, pterygoid plates, and temporalis at the tip of the coronoid, and high masseter involvement and retroantral fat pad were selected for ITF clearance. This objective criterion was used to reduce selection bias for ITF clearance. Patients with cT4b disease involving fewer than 3 structures were considered for standard composite resection with wide margins.
Exclusions –
1. Patients with carotid artery encasement, prevertebral fascia involvement, and Pterygomaxillary Fissure (PMF) widening on imaging.
2. Patients with distant metastasis.
3. Disease involving the temporal fossa/ significant disease above the sigmoid notch.
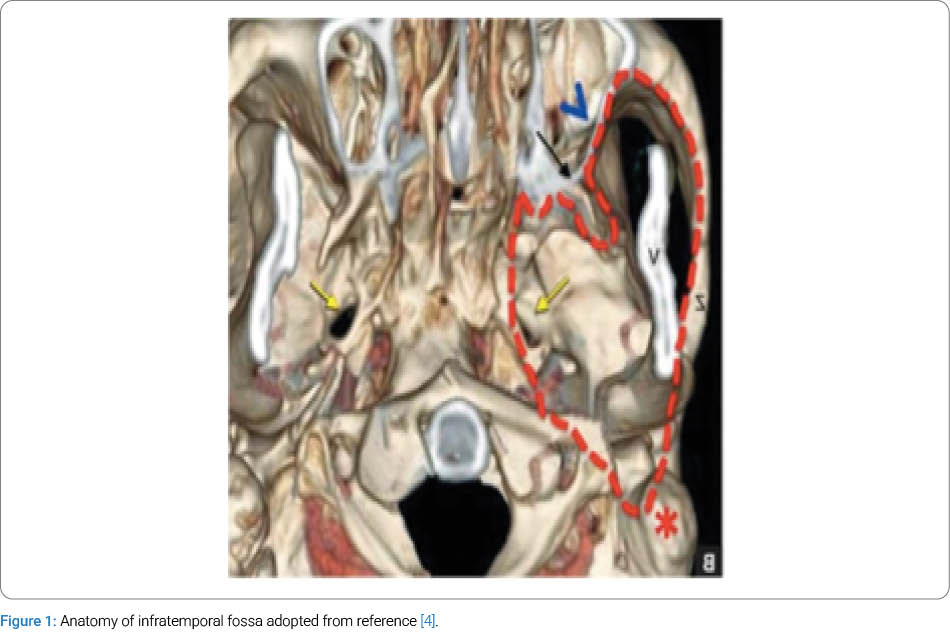
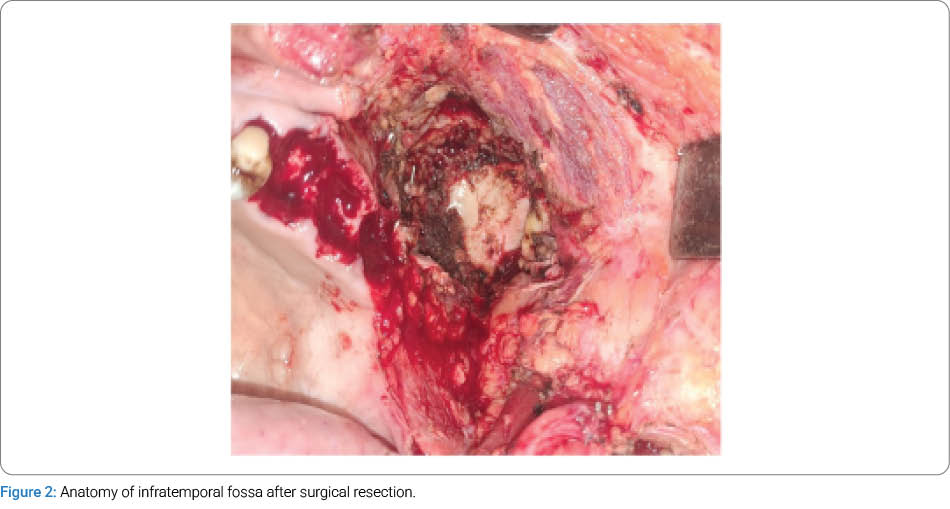
The patients were operated on per primum or after Neoadjuvant Chemotherapy (NACT). The patients who had skin oedema going beyond the zygoma superiorly or going to the parotid laterally were considered for NACT. All patients underwent a standardized surgical procedure of ITF compartmental clearance as defined in our last publication [3]. The boundaries of clearance were defined as follows: medially - the Eustachian tube; laterally - the capsule of TM joint; and superiorly - the greater wing of the sphenoid bone. All muscles, fibro-fatty tissue, and neurovascular bundle, retroantral fat, and pterygoid plates in that region were removed to achieve full clearance (Figure 1, Figure 2) [4]. All patients received adjuvant treatment (radiotherapy or chemo-radiation) as per the surgical histopathology report. Patients were followed up every 3 months for the first 2 years. After that, 6-monthly follow-ups were done according to institutional protocols. Radiological investigations were done on clinical suspicion of disease recurrence on follow-up.
Data were collected for baseline characteristics, clinical outcomes, complications, regional & locoregional recurrences, disease-specific survival, and overall survival. Overall Survival (OS) was calculated as the time interval between death due to any cause and the date of surgery; Disease-Free Survival (DFS) was calculated as the time interval between local, regional, or loco-regional recurrence, distant metastasis, or second primary and the date of surgery. Similarly, loco-regional control was calculated as the time interval between local or regional recurrence and the date of surgery. Death due to other causes was not counted for DFS, local control, and loco-regional control events. The appearance of skin nodules in the neck was considered a distant metastasis for estimating DFS. Prognostic variables were analysed using the log-rank test for univariate analysis and the Cox proportional hazards model for multivariate analysis. Survival analysis was done using the Kaplan-Meier survival estimate. P-values <0.05 were considered statistically significant, and graphical assessment of the data and all calculations were performed using SPSS 25 (SPSS Inc., 233, Chicago, Illinois, USA).
Results
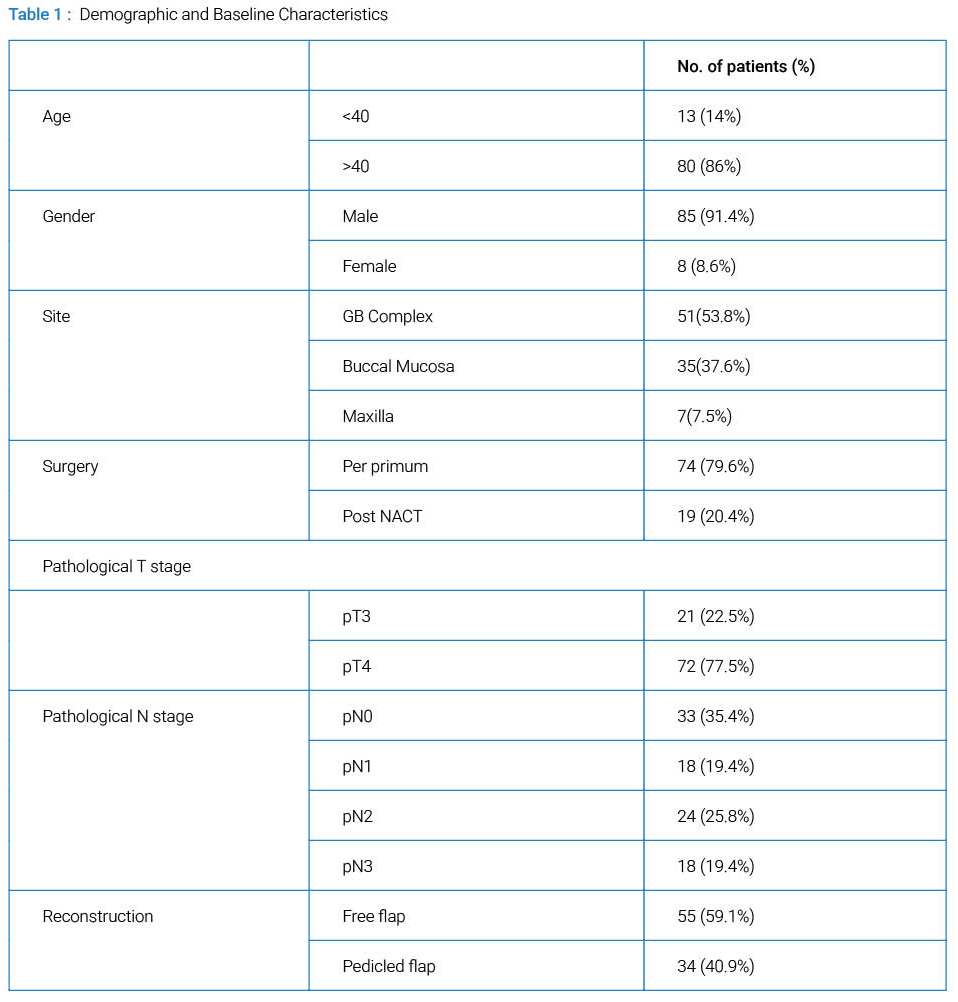
A total of 93 patients with an advanced subset of cT4b carcinoma of the oral cavity have been included in this retrospective analysis of prospectively maintained data of 1223 patients between 2013 and 2023. The majority of patients were more than 40 years of age (86%) with a median age of 50 years. 91.4% (85 patients) of the study population were male. The most common site of involvement was the GB complex (53.8%), followed by the buccal mucosa (37.6%) and the maxilla (7.5%). 79.6% patients underwent primary surgery, and 20.4% patients underwent neoadjuvant chemotherapy followed by surgery. Most patients were reported to be pT4 (77.5%), and 22.5% were pT3 on final histopathology. Around thirty-five percent (35.4%) of the study population was node negative, followed by pN1 (19.4%), pN2 (25.8%), and pN3 (19.4%). A total of fifty-nine patients (64.6%) had node-positive disease. The majority of patients underwent free flap reconstruction (59.1%), followed by pedicled flaps (40.9%). Other baseline characteristics, pathological tumour, and nodal stages are summarized in (Table 1).
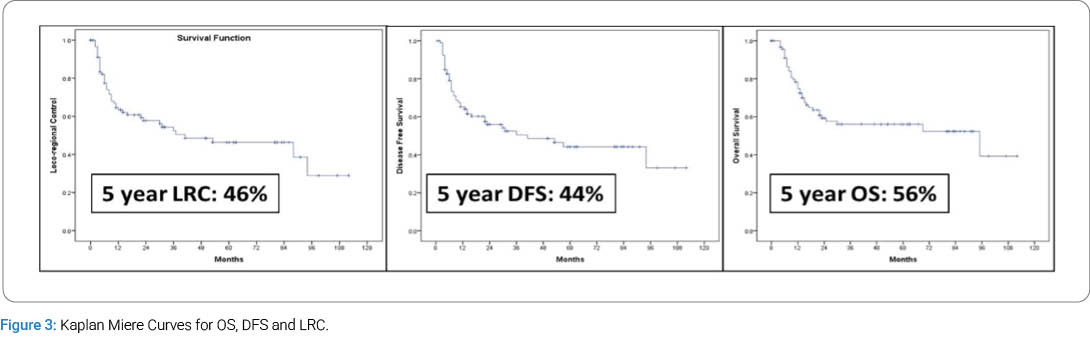
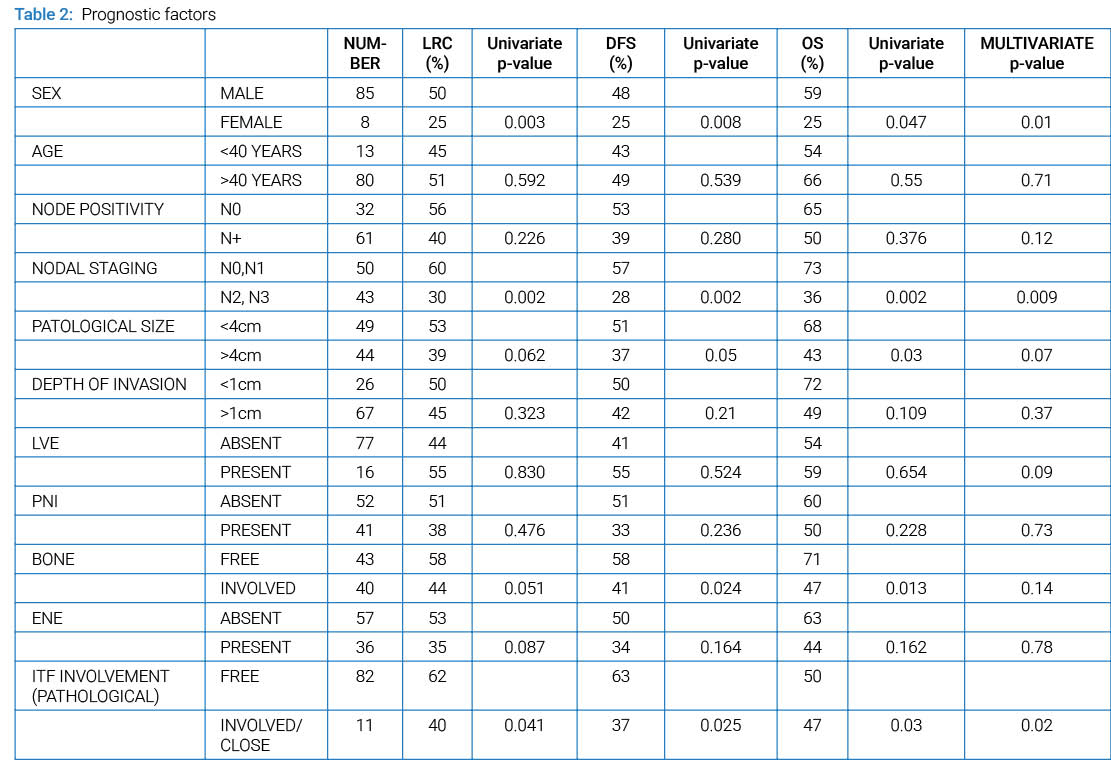
On the last follow-up, 55 of the 93 patients were alive. Forty-three patients had loco-regional recurrence (ITF recurrence 13), and 16 patients had distant metastasis. The median time for development of distant metastasis was 7 months (range 4 months–41 months). At median follow-up of 53 months (95% CI: 36 months–69 months), the 5-year LRC, DFS, and OS was 46%, 44%, and 56%, respectively (Figure 3). In multivariate analysis, the presence of advanced nodal disease and pathological ITF involvement was found to be significant for overall survival (Table 2). A Comparison of outcomes with our initial published analysis of 54 patients is given in (Table 3).

Discussion
Masticatory space and Infratemporal Fossa (ITF) are two synonymously used terms in clinical practice, frequently as misnomers. ITF is part of the masticatory space comprising the medial and lateral pterygoid muscle, the high masseter muscle, the temporalis at the tip of the coronoid, the pterygoid plates, retroantral fat, and a few neurovascular bundles arranged in multidimensional anatomy. According to the 8th edition AJCC staging, T4b denotes a tumour that involves the Masticator Space (MS), the Pterygoid Plates (PP), the skull base, or encases the internal carotid artery and represents very advanced disease with a poor prognosis [5]. The involvement of the infratemporal fossa is still deemed as borderline operable or non-operable. This is attributed to the complex anatomy, difficulty in attaining adequate margins, and a pre-conception of poor surgical outcomes. We have defined ITF clearance as the removal of contents of infratemporal fossa extending medially from pterygomaxillary fissure till ramus of mandible and TMJ laterally and superiorly till greater wing of sphenoid in our previous publication. Hereby, we present a long-term follow-up of our patients with clinico-radiological ITF involvement who were treated with ITF clearance.
The clearance of BM-GBS complex (buccal mucosa-gingiva buccal sulcus complex) tumours involves standard surgical clearance with >1 cm margins clinically around the disease. The difference from the standard technique in this advanced subset included a higher superior cut at the zygoma (if required, zygoma bone can also be taken into the specimen), so that the whole masseter muscle and temporalis beneath it at a higher level superiorly is included in the specimen. The posterior clearance is also done at the level of the greater wing of the sphenoid to make sure the whole pterygoid group of muscles is part of the surgical specimen. Pterygomaxillary fissure was identified, and fibrofatty tissue was cleared around it as well. There has been growing evidence regarding improved outcomes of ITF clearance in recent years. Many authors have shown improved survival after compartmental resection of ITF, especially in groups from the Indian subcontinent, where this disease is more prevalent [6–11]. The studies by Trivedi et al., [6,7] supported the concept that a group of patients with tumours with masticator space involvement can be treated likewise T4a tumours likewise. Previously, we published our clinical outcomes of 54 patients with a very advanced subset of cT4b carcinoma of buccal mucosa GB complex tumours treated surgically with compartment clearance of Infra-temporal fossa and found satisfying results [3]. At median follow-up of 29 months, we reported 2-year OS, DFS, and LRC at 54%, 54%, and 52%, respectively. Perineural invasion, pathological tumour stage, node positive, and ITF tissue involvement were associated with poor oncological outcomes. In this study, we did a 5-year analysis with an increased sample size (93) with a median follow-up of 53 months. Five-year OS, DFS, and LRC was 56%, 44.1%, 46% respectively, which, looking at this subset of very advanced cT4b BM-GBS complex, is highly encouraging.
There is still a dearth of studies examining advanced subsets of cT4b disease outcomes following compartmental clearance of ITF. Pillai et al. had reclassified cT4b disease into type I/II/III depending on the anatomical involvement of structures in the ITF region [8]. They reported a higher risk of locoregional recurrence in the type II/III group, as expected. Their intermediate group that is type II correlates with our dataset as per anatomical similarities, though their number (n = 28) was pretty small compared to our larger cohort of 93 patients. They reported poor DFS in type II compared to type I lesions, though not significant on univariate and multivariate analysis. Our 2-year survival outcomes were similar to Pillai et al.’s type II group (DFS 54% vs 51%). Similarly, other groups who have reported similar outcomes with ITF clearance had smaller numbers compared to our cohort [9–11]. Now, with 5-year survival outcomes and a larger cohort, we believe that at present our data is the largest in the world in this context, with a longer duration of follow-up.
A recent Meta-analysis of Surgical Outcomes of Infranotch T4b Oral Cancers by Karthik N rao et al., [12] observed pooled 2 and 5 year overall survival (OS) at 59.3% and 53.2%, 2 and 5 year Disease-Free Survival (DFS) 57.9% and 48.4%, 2 and 5 year disease-specific survival (DSS) 72% and 68%, and 2 and 5 year Local Control (LC), 47% and 56%, respectively which is nearly similar to our results despite our cohort having more locally advanced disease. The difficulty in achieving clear margins is one of the arguments given against surgical clearance of disease involving ITF. We reported close or positive margins in approximately 28 of patients (n = 27; close 19, positive 8) and, as expected, observed a significant impact on overall survival (p = 0.016), d isease-free survival (p = 0.047), and loco-regional control (p = 0.037). A close or positive margin in this region is important, as the close proximity of various foramina foramina at the skull base provides a route for disease spread and, subsequently, local recurrence.
Advanced nodal disease among ITF patients is associated with poor overall survival, disease-free survival, and locoregional control, and patients with perinodal extension had worse survival among this subset [3]. In our dataset, bulky nodal disease (N2, N3) was a significant prognostic factor for LRC, DFS, and OS on univariate and multivariate analysis (p = 0.009). The other issue authors feel is the reporting of histopathological specimens. The muscles of mastication are clubbed and reported together, which we think doesn’t accurately represent the extension of the disease. The tagging of muscles (pterygoids, masseter, and temporalis) in a prospective setting would give a better idea of masticatory muscle infiltration and improve pathological staging of disease. The strength of this study is the uniform surgical technique and long follow-up of patients. At the same time, all cases were operated by a single surgical team with a pretty standardized technique of ITF clearance. Formal quality-of-life assessment is not conducted, as this is a retrospective analysis. We intend to analyse the quality of life in this group of patients in the future cohort.
Conclusion
Compartmental ITF clearance provides a curative option for long-term survival for T4b oral cavity cancers with good 5-year OS and DFS. Good margin clearance, if achievable, and nodal staging are important predictors of outcomes. Involvement of the pterygoid muscles at the source of origin has a higher risk of local recurrence. Node-negative disease in this advanced cohort has the best outcomes. Compartment clearance of ITF in very advanced T4b should be the norm, not an exception, provided good patient selection.
References
- Liao CT, Ng SH, Chang JT, Wang HM, Hsueh C, Lee LY, et al. T4b oral cavity cancer below the mandibular notch is resectable with a favorable outcome. Oral Oncol. 2007;43(6):570–579.
- Liao CT, Chang JTC, Wang HM, Ng SH, Hsueh C, Lee LY, et al. Surgical outcome of T4A and resected T4B oral cavity cancer. Cancer. 2006;107(2):337–344.
- Katna R, Kalyani N, Singh S, Bhosale B; Mumbai Oncology Group – Head and Neck. Compartmental clearance of infratemporal fossa for T4B carcinoma of buccal mucosa/alveolus: Clinical outcomes. Indian J Surg Oncol. 2020;11(2):316–320.
- Arya S, Rane P, D’Cruz A. Infratemporal Fossa, Masticator Space and Parapharyngeal Space: Can the Radiologist and Surgeon speak the Same Language? Int J Otorhinolaryngol Clin. 2012;4(3):125–135.
- Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC cancer staging manual 7th Editon. Springer. 2018.
- Trivedi NP, Kekatpure V, Kuriakose MA. Radical (compartment) resection for advanced buccal cancer involving masticator space (T4b): our experience in thirty patients. Clin Otolaryngol. 2012;37(6):477–483.
- Trivedi NP, Kekatpure VD, Shetkar G, Gangoli A, Kuriakose MA. Pathology of advanced buccal mucosa cancer involving masticator space (T4b). Indian J Cancer. 2015;52(4):611–615.
- Pillai V, Yadav V, Kekatpure V, Trivedi N, Chandrashekar NH,Shetty V, et al. Prognostic determinants of locally advanced buccal mucosa cancer: Do we need to relook the current staging criteria? Oral Oncol. 2019:95:43–51.
- Mohiyuddin SMA, Harsha P, Maruvala S, Sumanth KR, Suresh TN, Manjunath GN, et al. Outcome of compartment resection of locally advanced oral cancers extending to infratemporal fossa: a tertiary rural hospital experience. Eur Arch Otorhinolaryngol. 2018;275(11):2843–2850.
- Mishra P, Hadi R, Gandhi AK, Rastogi M, Khurana R, Singhal A, et al. Prospective Evaluation of Locoregional Control in Oral Cavity Squamous Cell Carcinoma with Infratemporal Fossa Involvement Treated with Surgery and Adjuvant Concurrent Chemoradiotherapy. Int J Radiation Oncology Biology Physics. 2023;117(2):E607.
- An Kumar N, Dikhit PS, Rajan K, Usman N, Shetty PS, Mehta V, et al. Enbloc resection of primary oral cancer involving infratemporal fossa: A systematic “out to in and top to bottom” surgical approach and outcomes, J Stomatol Oral Maxillofac Surg. 2023;124(6S):101515.
- Rao KN, Arora R, Dange P, Nagarkar N, Mäkitie AA, Kowalski LP, et al. A Meta-analysis of Surgical Outcomes of T4a and Infranotch T4b Oral Cancers. Oncol Ther. 2023;11(4):461–480.
Cite this article
Katna R, Maini A, Chalke S, Paatni P, Bhosale B, Patil V, et al. Mumbai Oncology Group – Head and Neck. Long term clinical outcomes of Compartmental Clearance of Infratemporal Fossa in very advanced subset of cT4b Carcinoma of Buccal Mucosa- Gingivo Buccal complex. Clin Oncol J. 2026;7(2):1–6.
Keywords
Infratemporal fossa clearance; T4b carcinoma oral cavity; Bite composite resection
Copyright
© 2026 Koch BA. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
