Prognostic Role of the Mismatch Repair Deficiency in Patients with Endometrial Cancer Receiving Radiotherapy
* Abdurahman Kuzhan;
-
* Abdurahman Kuzhan: Department of Radiation Oncology, Faculty of Medicine, Gaziantep University, Gaziantep, Turkey
Abstract
Aim: Mismatch repair deficiency is an important prognostic subgroup of endometrial cancer. which is detected in approximately one-third of patients with endometrial cancer. Mismatch repair proteins play a role in DNA repair after radiation therapy. We investigated the mismatch repair status as a predictor of radiotherapy response in the adjuvant setting of patients with endometrial cancer.
Methods: We included 165 patients diagnosed with endometrial cancer and referred to the Oncology Hospital for radiotherapy. We analyzed the association between mismatch repair deficiency and clinical parameters with a chi-square test. We evaluated the prognostic significance of mismatch repair deficiency using Kaplan–Meier survival analysis and log-rank tests.
Results: Median follow-up was 4.5 years (range, 0.4–5.7 years). Of the 165 patients, 61 (37%) were mismatch repair deficiency. Survival did not differ between mismatch repair deficiency and MMR-normal groups. Mismatch repair deficiency status also did not affect survival in patients who received or did not receive radiotherapy.
Conclusion: Although several studies have reported that mismatch repair status may be an effective marker in the prediction of the response to adjuvant radiotherapy in endometrial cancer patients, we could not find evidence supporting that in this study.
Abbreviations
MMR: mismatch repair; MMRd: mismatch repair deficiency; MMRn: mismatch repair normal; MSI: microsatellite instability; IHC: immunohistochemistry; EC: endometrial cancer; OS: overall survival; PFS: progression-free survival; DFS: disease-free survival; LVSI: lymphovascular space invasion; LNM: lymph node metastasis; RT: radiotherapy; PCR: polymerase chain reaction; POLE: DNA polymerase epsilon; TCGA: The Cancer Genome Atlas; FIGO: International Federation of Gynecology and Obstetrics
Introduction
Endometrial cancer (EC) was diagnosed in 417,367 women worldwide, and it is estimated that 97,370 women died from EC according to data from 2020 [1]. EC is commonly diagnosed at an early stage of the disease, which is associated with a better prognosis, with a 5-year survival rate of 95%. At advanced stages, particularly in metastatic disease, survival decreases to 17% [2,3]. Pathologic type, histologic grade, lymphovascular involvement, and tumor stage have previously been studied for their prognostic effects on EC; however, their prognostic effects remain unclear. Therefore, recent studies have focused on gene carcinogenesis (i.e., molecular alterations) to provide an actual prognostic classification.
The mismatch repair (MMR) system increases the fidelity of replication by promoting DNA repair with the mechanisms of excision and resynthesis [4]. Mismatch repair deficiency (MMRd) may be inherited or acquired and occurs in approximately 20% to 40% of EC patients [5–9]. MMRd can be defined as the detection of Microsatellite Instability (MSI) or Immunohistochemical (IHC) loss of one or more of the MMR proteins (MLH1, PMS2, MSH2, and/or MSH6).
Four molecular prognostic groups were described by the Proactive Molecular Risk Classifier for Endometrial Cancer (ProMisE) in 2017. These groups are classified as ultra-mutated DNA polymerase epsilon (POLE), MSI or MMR hypermutated tumors, p53 abnormal tumors, and tumors with copy-number low alterations, and these groups are associated with the best prognosis, intermediate prognosis, the worst prognosis, and good to intermediate prognosis, respectively [10]. This classification was reported to be applied to a practical approach to EC patients and is accepted to be consistent with The Cancer Genome Atlas (TCGA) [11,12].
In addition to MMR testing, IHC markers such as p53 or POLE have been recommended to be placed in a diagnostic algorithm [13] to determine risk groups, and are currently included in the latest European Society of Gynecological Oncology/European Society for Radiotherapy (RT) and Oncology/European Society of Pathology (ESGO/ESTRO/ESP) [14]. The National Comprehensive Cancer Network has recommended the universal testing of all ECs for MSI/MMRd status since 2018 [15]. IHC is commonly used by oncologic centers for testing because it is inexpensive and has high sensitivity, specificity, and reproducibility [11,16]. Currently, prediction of the response to RT with markers is needed to decide which patients may benefit from RT. So far, the effect of MMRd on the prognosis of patients with EC treated with RT has been evaluated in a few studies [17,18], and its role in prognosis remains unclear. In this retrospective study, the relationship between MMR and prognostic factors and the effect of MMR on prognosis in patients with EC who received RT were analyzed.
Material and Methods
A total of 165 patients who were diagnosed with EC and referred to the Oncology Hospital for RT between January 2010 and July 2022 were included in the study. The retrospective study was approved by the local ethics board and conducted in accordance with the principles of the 2013 Helsinki Declaration.
The surgical procedure performed was a total abdominal hysterectomy and bilateral salpingo-oophorectomy, with or without pelvic and paraaortic lymphadenectomy. For inclusion, patients either received adjuvant RT or did not receive any treatment. As a result, after excluding the 49 patients who received chemotherapy alone or RT combined with chemotherapy, the number of patients decreased to 165. Data recorded included histology, grade, lymph node status, International Federation of Gynecology and Obstetrics (FIGO) stage (2009), depth of myometrial invasion, and lymphovascular invasion. Additionally, patients were grouped into low- and high-risk categories based on prognostic factors.
Two equivalent screening methods are widely accepted to assess MMR deficiency: Polymerase chain reaction (PCR)-based microsatellite instability and Immunohistochemistry (IHC) for loss of MLH1, MSH2, MSH6, or PMS2. The agreement between both methods is excellent (> 90%) [19]. We chose IHC because it is more accessible and inexpensive, and it provides stringent inter-laboratory quality assurance [19]. MLH1, MSH2, MSH6, and PMS2 protein expressions were considered lost when less than 5% of tumor cells stained positive in the presence of an internal positive control of normal lymphocytes and/or stromal cells [20]. MMR deficiency (MMRd) was defined as the presence of at least one MMR protein loss in the tumor.
Overall survival (OS) was defined as the time from the date of diagnosis until last follow-up or death. Progression-free survival (PFS) was defined as the time from the date of diagnosis to the date of progression, the end of the follow-up period, or death. SPSS (Statistical Package for Social Sciences) for Windows 23.0; IBM SPSS Statistics, New York, USA, was used for statistical analyses. The association between MMRd and clinical parameters was analyzed with a chi-square test. The prognostic significance of MMRd was evaluated using Kaplan–Meier survival analysis and log-rank tests. The significance level was set at 5%.
Results
Among the 165 patients analyzed, 61 (37%) were considered MMRd. The remaining patients (n = 104) were MMR normal (MMRn). Loss of MLH1, MSH2, MSH6, and PMS2 expression was detected in 36 (21.8%), 59 (35.8%), 56 (33.9%), and 35 cases (21.2%), respectively. The association between MMR status and clinical parameters is summarized in (Table). There was a statistically significant association between MMRd and grade (p < 0.04), advanced stage (p < 0.02), lymphovascular space invasion (LVSI) (p < 0.04), or paraaortic nodal metastasis (p < 0.03). However, no significant relationship was found between MMRd and histology, risk groups, or lymph node metastasis (LNM) (p > 0.1).
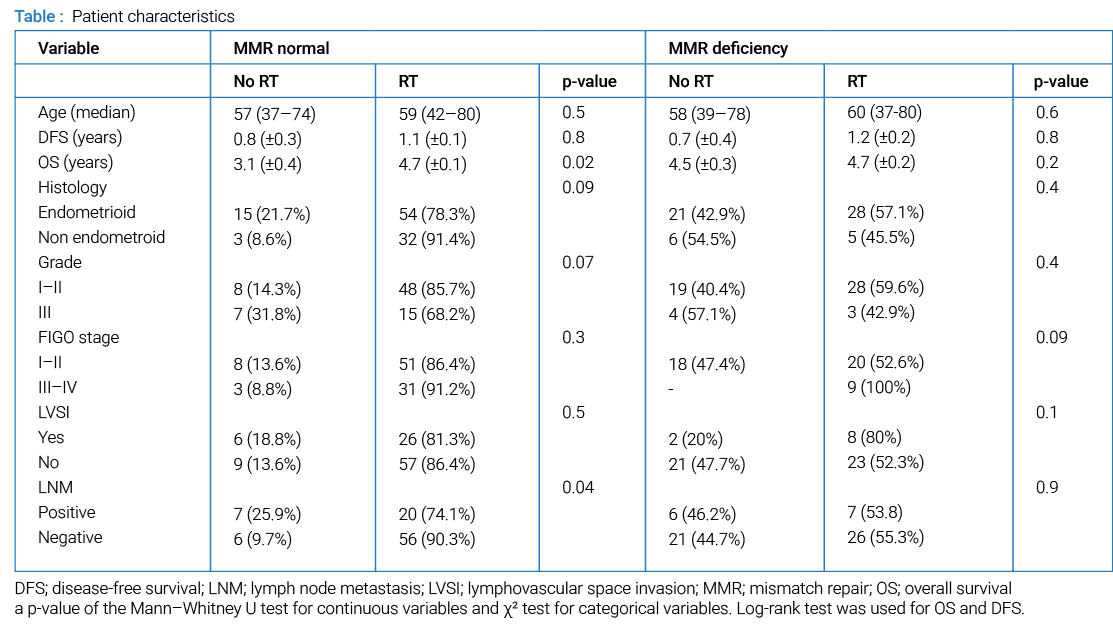
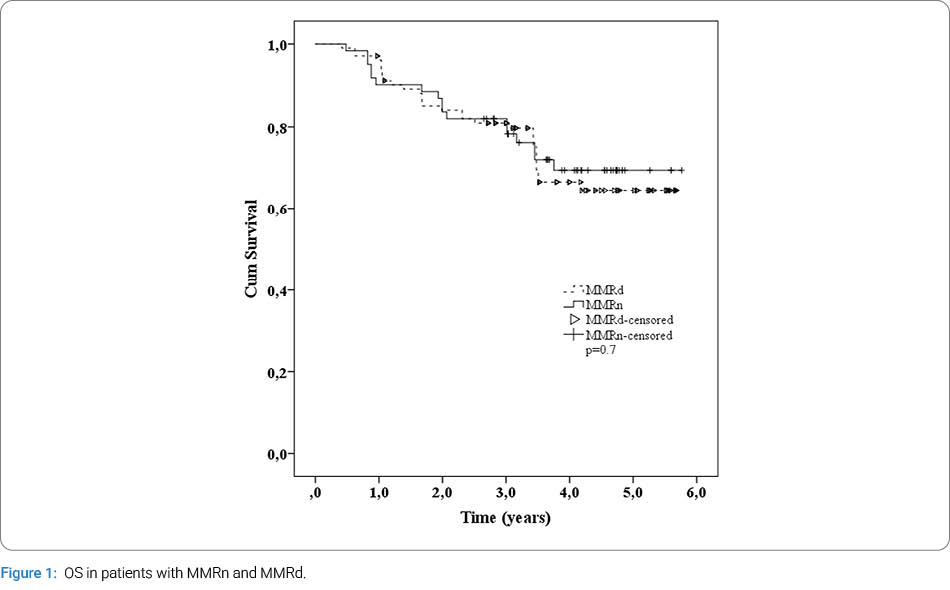
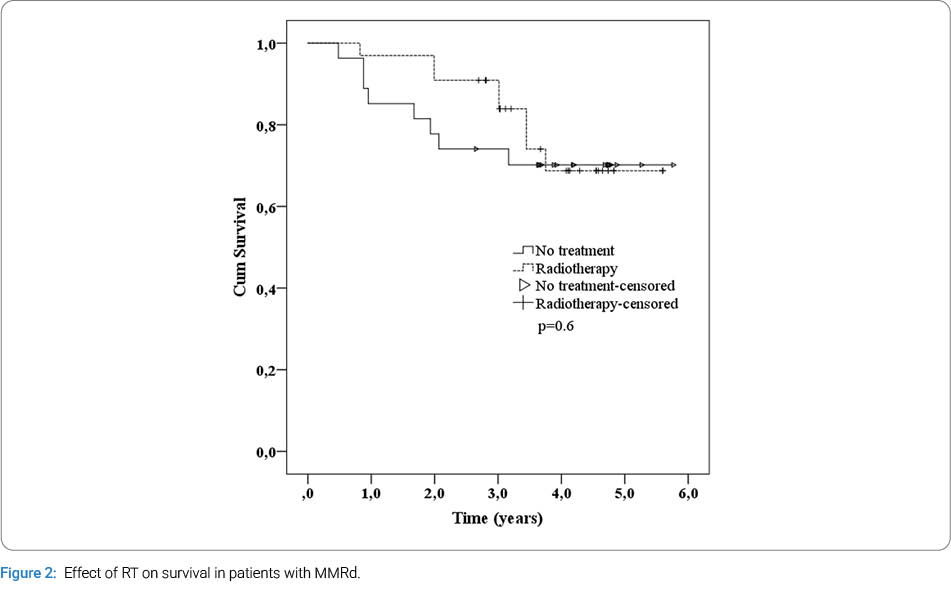
Median age was 59 years (range, 37–80 years), and median follow-up time was 4.5 years (0.4–5.7 years) (Table). No survival difference was found between MMRd and MMRn by the log-rank test. OS was found to be 4.65 and 4.5 years in patients with MMRd and MMRn, respectively (Figure 1). Moreover, no effect of MMRd on survival was found in patients who were treated with or without RT (Figure 2). Additionally, in patients with MMRd tumors who received RT, prognostic factors did not have an effect on OS and DFS (p > 0.5).
Discussion
Previous studies have shown that, in women with EC, DNA MMR modulates chemotherapy or RT responses in certain patient subgroups and that MMR status has prognostic significance [17,18,21]. Contrary to these studies, this study found no effect of MMR status on prognosis in patients receiving RT. The MMRd tumor phenotype represents 20%–40% of all ECs. This specific molecular genetic alteration, resulting from a defect in the MMR genes MLH1, MSH2, MSH6, or PMS2, is found in both sporadic tumors and those associated with Lynch-like syndrome [5,9]. The accumulation of nucleotide insertions or deletions within coding repeat sequences increases lymphocyte infiltration, thereby facilitating immunotherapy [22]. Therefore, it is crucial to identify MMRd tumors for the management of EC patients and for prognostic prediction.
Endometrial tumors with DNA MMRd were found to be associated with poor prognostic factors, including lymphovascular space invasion and cervical involvement, in the previous study. MMRd tumors were reported to be related to worse survival when compared with MMRn tumors [21]. However, unlike the reported findings, we did not find an association in our study. However, in patients with MMRd, lymphovascular space involvement was less common, whereas metastatic disease was more common. Nevertheless, we could not detect any effect of these prognostic factors on OS in patients with MMRd treated with RT.
In the previous studies, grade 3 tumors were reported to be more frequent in patients with MMRd, and consequently, these patients had a worse prognosis [23]. In the present study, the rate of grade 3 tumors was lower in patients with MMRd, but this did not affect prognosis. Regarding the risk groups determined by prognostic factors, patients with MMRd were reported to be associated with HIR. Additionally, the prognosis of patients with MMRd in the LIR and HIR risk groups has been reported to be worse [23]. However, such a relationship and poorer prognosis were not found in this study.
Conclusion
Although several studies have reported that MMR status may be an effective marker for predicting response to adjuvant RT in EC patients, we did not find evidence supporting this in this study. Prospective randomized studies are needed to elucidate this issue.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA cancer J Clin. 2021;71(3):209–249.
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33.
- American Cancer Society. Cancer facts & figures 2022 [Internet]. New York: American Cancer Society; 2022.
- Reyes GX, Schmidt TT, Kolodner RD, Hombauer H. New insights into the mechanism of DNA mismatch repair. Chromosoma. 2015;124(4):443–462.
- Kim SR, Pina A, Albert A, McAlpine J, Wolber R, Blake Gilks C, et al. Does MMR status in endometrial cancer influence response to adjuvant therapy? Gynecol Oncol. 2018;151(1):76–81.
- Pina A, Wolber R, McAlpine JN, Gilks B, Kwon JS. Endometrial cancer presentation and outcomes based on mismatch repair protein expression from a population-based study. Int J Gynecol Cancer. 2018;28(8):1624–1630.
- Talhouk A, McConechy MK, Leung S, Li-Chang HH, Kwon JS, Melnyk N, et al. A clinically applicable molecular-based classification for endometrial cancers. Br J Cancer. 2015;113(2):299–310.
- Kommoss S, McConechy MK, Kommoss F, Leung S, Bunz A, Magrill J, et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann Oncol. 2018;29(5):1180–1188.
- Mc Meekin DS, Tritchler DL, Cohn DE, Mutch DG, Lankes HA, Geller MA, et al. Clinicopathologic significance of mismatch repair defects in endometrial cancer: an NRG Oncology/Gynecologic Oncology Group study. J Clin Oncol. 2016;34(25):3062–3068.
- Talhouk A, Mc Conechy MK, Leung S, Yang W, Lum A, Senz J, et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer. Cancer. 2017;123(5):802–813.
- Travaglino A, Raffone A, Mascolo M, Guida M, Insabato L, Zannoni GF, et al. Clear cell endometrial carcinoma and the TCGA classification. Histopathology. 2020;76(2):336–338.
- Cancer Genome Atlas Research Network; Kandoth C, Schultz N, Cherniack AD, Akbani R, Liu Y, Shen H, et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67–73.
- Vermij L, Smit V, Nout R, Bosse T. Incorporation of molecular characteristics into endometrial cancer management. Histopathology. 2020;76(1):52–63.
- Concin N, Matias-Guiu X, Vergote I, Cibula D, Mirza MR, Marnitz S, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12–39.
- Koh WJ, Abu-Rustum NR, Bean S, Bradley K, Campos SM, Cho KR, et al. Uterine neoplasms, version 1.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2018;16(2):170–199.
- Raffone A, Travaglino A, Cerbone M, Gencarelli A, Mollo A, Insabato L, et al. Diagnostic accuracy of immunohistochemistry for mismatch repair proteins as surrogate of microsatellite instability molecular testing in endometrial cancer. Pathol Oncol Res. 2020;26(3):1417–1427.
- Reijnen C, Küsters-Vandevelde HVN, Prinsen CF, Massuger LFAG, Snijders MPML, Kommoss S, et al. Mismatch repair deficiency as a predictive marker for response to adjuvant radiotherapy in endometrial cancer. Gynecol Oncol. 2019;154(1):124–130.
- Resnick KE, Frankel WL, Morrison CD, Fowler JM, Copeland LJ, Stephens J, et al. Mismatch repair status and outcomes after adjuvant therapy in patients with surgically staged endometrial cancer. Gynecol Oncol. 2010;117(2):234–238.
- Clarke BA, Cooper K. Identifying Lynch syndrome in patients with endometrial carcinoma: shortcomings of morphologic and clinical schemas. Adv AnatPathol. 2012;19(4):231–238.
- Watkins JC, Nucci MR, Ritterhouse LL, Howitt BE, Sholl LM. Unusual mismatch repair immunohistochemical patterns in endometrial carcinoma. Am J Surg Pathol. 2016;40(7):909–916.
- Cohn DE, Frankel WL, Resnick KE, Zanagnolo VL, Copeland LJ, Hampel H, et al. Improved survival with an intact DNA mismatch repair system in endometrial cancer. Obstet Gynecol. 2006;108(5):1208–1215.
- Ono R, Nakayama K, Nakamura K, Yamashita H, Ishibashi T, Ishikawa M, et al. Dedifferentiated endometrial carcinoma could be a target for immune checkpoint inhibitors (anti PD-1/PD-L1 antibodies). Int J Mol Sci. 2019;20(15):3744.
- Li JY, Park HS, Huang GS, Young MR, Ratner E, Santin A, et al. Prognostic impact of mismatch repair deficiency in high- and low-intermediate-risk, early-stage endometrial cancer following vaginal brachytherapy. Gynecol Oncol. 2021;163(3):557–562.
Cite this article
Kuzhan A. Prognostic role of the mismatch repair deficiency in patients with endometrial cancer receiving radiotherapy. Clin Oncol J. 2026;7(2):1–5.
Keywords
Endometrial cancer; Mismatch repair deficiency; Radiotherapy
Copyright
© 2026 Abdurahman Kuzhan. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
