Abstract
Primary immune deficiencies, also known as Inborn Inborn errors of immunity, are a large family of genetically characterized diseases that compromise innate and adaptive immunity. Susceptibility to infections, autoimmunity, autoinflammatory and allergic diseases, and the occurrence of malignancies characterize the evolution of these diseases. In this mini-review, we attempt to describe the types of malignancies associated with Inborn errors of immunity, their likely mechanisms of occurrence, methods for diagnosing them as early as possible, and current and future therapeutic methods for treating them.
Inborn errors of immunity patients have a many-fold increased risk to develop malignancies, appearing generally at earlier ages and dominated by lymphomas characterized by a rapid clinical progression, polymorphic cell population, Epstein–Barr virus association, and significant morbidity and mortality risks. Many mechanisms drive Inborn errors of immunity towards malignant transformation. Some depending on Inborn errors of immunity intrinsic dysfunction and other extrinsic factors due to transforming viral infections and chronic inflammation. Because of the high clinical variability and genetic heterogeneity for most Inborn errors of immunity, high-throughput sequencing methods or next-generation sequencing are increasingly used.
The most efficient treatment should provide a positive balance for immune protection in normal cells, while killing more malignant cells. Hematopoietic stem cell transplantation with reduced-intensity conditioning seems more effective in several disorders, with improved post-transplantation survival. Several gene therapy clinical trials are currently running for many inborn errors of immunity. Particularly, Autologous hematopoietic stem cell gene therapy.
As malignancies in the Inborn errors of immunity context set some diagnostic and therapeutic challenges (early identification, management of complications associated with treatments, and long-term follow-up and post-treatment monitoring), advances in diagnosis research and treatment will enable the management of Inborn errors of immunity and associated malignancies through targeted therapies: immunotherapy, personalized approaches based on the child’s genetic and immune profile, as well as gene therapies.
Conclusion: Education of physicians about the risk of malignancies during childhood in Inborn errors of immunity will accelerate diagnosis, personalize treatment, and ultimately improve outcomes in the future.
Introduction
Primary immune deficiencies (PID), also known as Inborn Errors of Immunity (IEI), are a large family of 485 genetically characterized diseases that compromise innate and adaptive immunity. They can be dominantly or recessively inherited, autosomal, or X-linked, and with complete or incomplete penetrance of the clinical phenotype. Susceptibility to infections, autoimmunity, autoinflammatory and allergic diseases, and the occurrence of malignancies characterize these diseases [1].
In this mini-review, we present the basis for the increased susceptibility to certain malignancies in children affected by certain types of IEI. We discuss the clinical, biological, and epidemiological features of these tumors. We also highlight new diagnostic methods, treatments, and practical recommendations for the management of these patients. We conclude with a critical analysis of this “IEI and malignant tumor” entity, in the light of spectacular advances in the diagnosis and treatment of IEI.
In their meta-analysis, Kindle et al. [2] reported that malignancies were among the first manifestations of IEI in 479 patients, and the only initial manifestation in 117 patients based on a panel of 30,628 patients of the European Society for Immunodeficiencies patient registry (ESID-R).
The type of malignancy is highly dependent on the IEI. In their review, Tiri et al. [3] report on the malignancy profiles of various subtypes of primary immunodeficiency. Thus, cancers overexpressed respectively in selective IgA deficiency, Common variable immunodeficiency (CVID), X-linked agammaglobulinemia (XLA), gastric cancers and lymphoma, Lymphoma, more frequently non-Hodgkin lymphoma (NHL) and (gastric, thymic, cervical) cancers, gastric and colorectal cancers, etc.
The underlying mechanisms for malignancies are largely unknown, although many causative genes were identified [4]. Many mechanisms can lead to malignant transformation in IEIs. Since the immune system plays a vital role in monitoring and combating malignant transformations, any anomaly or deficiency in it can lead to tumor escape. The mechanisms responsible for certain IEI are themselves linked to the specific immune defect, which are called intrinsic mechanisms: DNA breakage disorders in Ataxia Telangiectasia (AT) or Bloom’s Syndrome (BS), errors in cell apoptosis, abnormalities involving cell development and/or signaling, actin cytoskeleton, cytotoxicity, DNA repair, chromosome instability, and telomere maintenance [5–7]. Extrinsic mechanisms such as viral infections (Epstein–Barr virus (EBV), Human papillomavirus), chronic tissue inflammation, and impaired immune surveillance, which all increase oncogenic risk outside of the primary immune defect [7,8].
However, in a recent study, Bakhuizen et al. [9] were able for the first time to assess impartially and comprehensively the role of IEI/IBMFS (hereditary bone marrow failure syndromes) in predisposition to hematological malignancies in children. Several cohort studies have shown a higher incidence of malignancy in IEIs with approximately a 1.4-fold to 5-fold increase compared to the age-adjusted general population [10,11].
Several types of malignancies can be declared in IEI context, as leukemia, gastrointestinal cancers, cancers of the head and neck, breast cancers etc. [3,12], but lymphomas are the most frequently encountered tumor pathology in IEI, mainly large B-cell NHL, with a high grade of malignancy and EBV-induced lymphoproliferative diseases [6,7,13]. There is a 50-fold risk compared with the general population of developing any cancer, and up to 250-fold risk of lymphomas, predominantly NHL [14].
Malignancies in the IEI context set some diagnostic and therapeutic challenges as early identification of cancers, management of complications associated with anti-cancer treatments, and long-term follow-up and post-treatment monitoring. Advances in research and treatment will enable the management of IEI and associated malignancies through targeted therapies: immunotherapy, personalized approaches based on the child’s genetic and immune profile, as well as gene therapies [15].
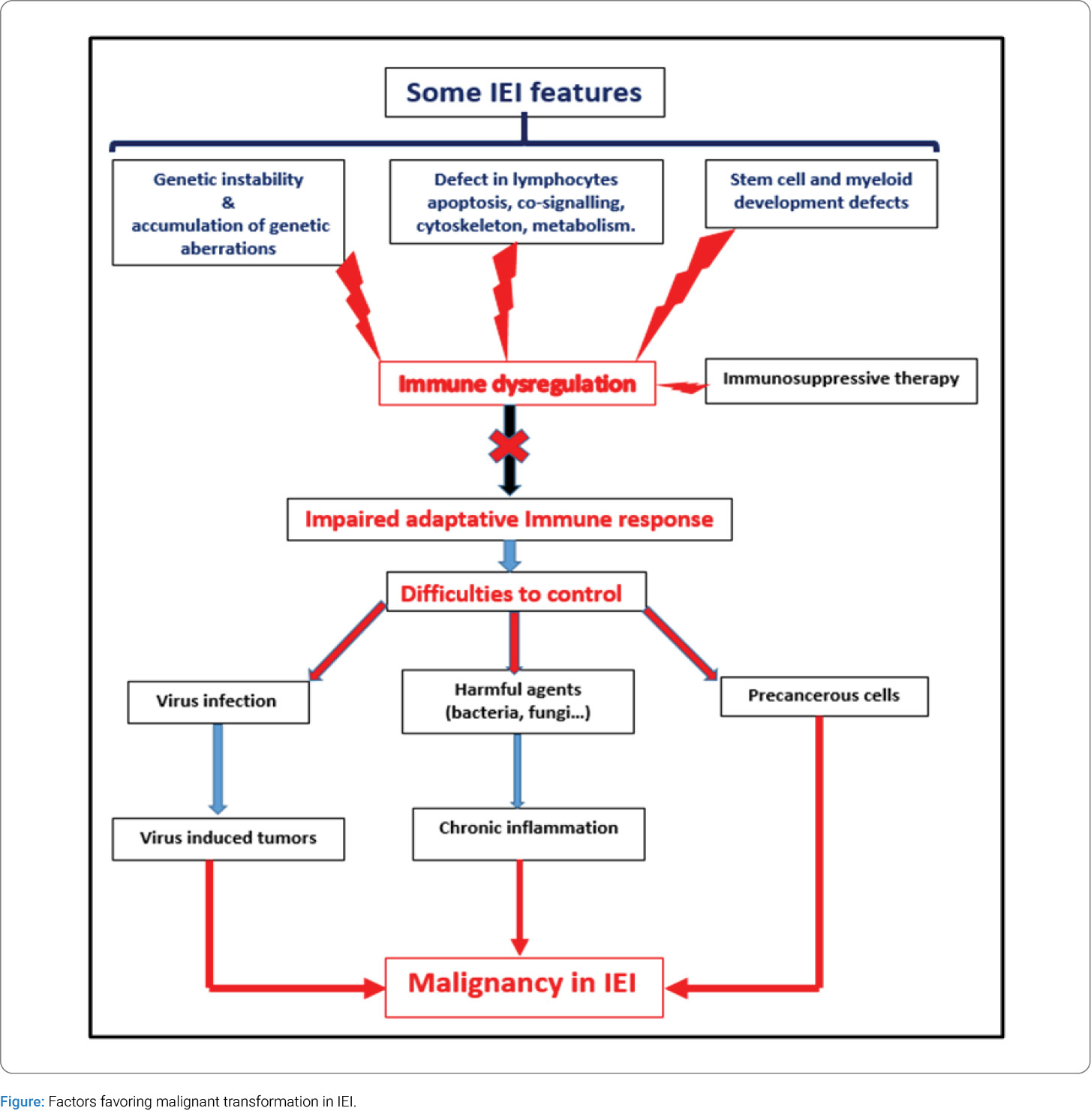
1. Why is there an increased susceptibility to cancer in IEI? (Figure)
Several mechanisms can explain the occurrence of malignancies in patients with IEI. Some are due to the pathology itself; these disorders arise from defects in differentiation or apoptosis, including cytoskeleton, lymphocyte co-signaling, metabolism, cytotoxicity, and impairment of the genetic material, including chromosome stability, telomere maintenance, and DNA repair. Cellular immunity, which is essential for tumor surveillance, is severely impaired in cases of combined immunodeficiency, where these lymphocytes are either absent, very few in number, and/or poorly functional [5,7].
Other causes include transforming infections, Epstein–Barr Virus (EBV), and Human Papillomavirus (HPV) infections, and chronic tissue inflammation. Antigen persistence in the body due to impairment of the immune system is responsible for chronic inflammation, causing tissue damage, which can lead to malignant transformation as seen with oncogenic viruses [7,8,16]. The chronic presence of these viruses causes cytokines production that promotes ectopic proliferation of lymphoid tissue [17]. Continuous antigenic stimulation resulted in a progressive loss of cytokine secretion (interleukin [IL]-2 and tumour necrosis factor [TNF]-α), impairment of interferon (IFN)-γ production, and premature apoptosis of CD8+ T cells [18]. This quantitative and qualitative loss of the CD8+ T cell immune responses against tumour cells can eventually result in the development of malignancy, being specifically recognized by T lymphocytes.
An iatrogenic mechanism can also contribute to the development of malignancies in these patients, namely the various immunosuppressive treatments given as part of the treatment to stem the chronic inflammation.
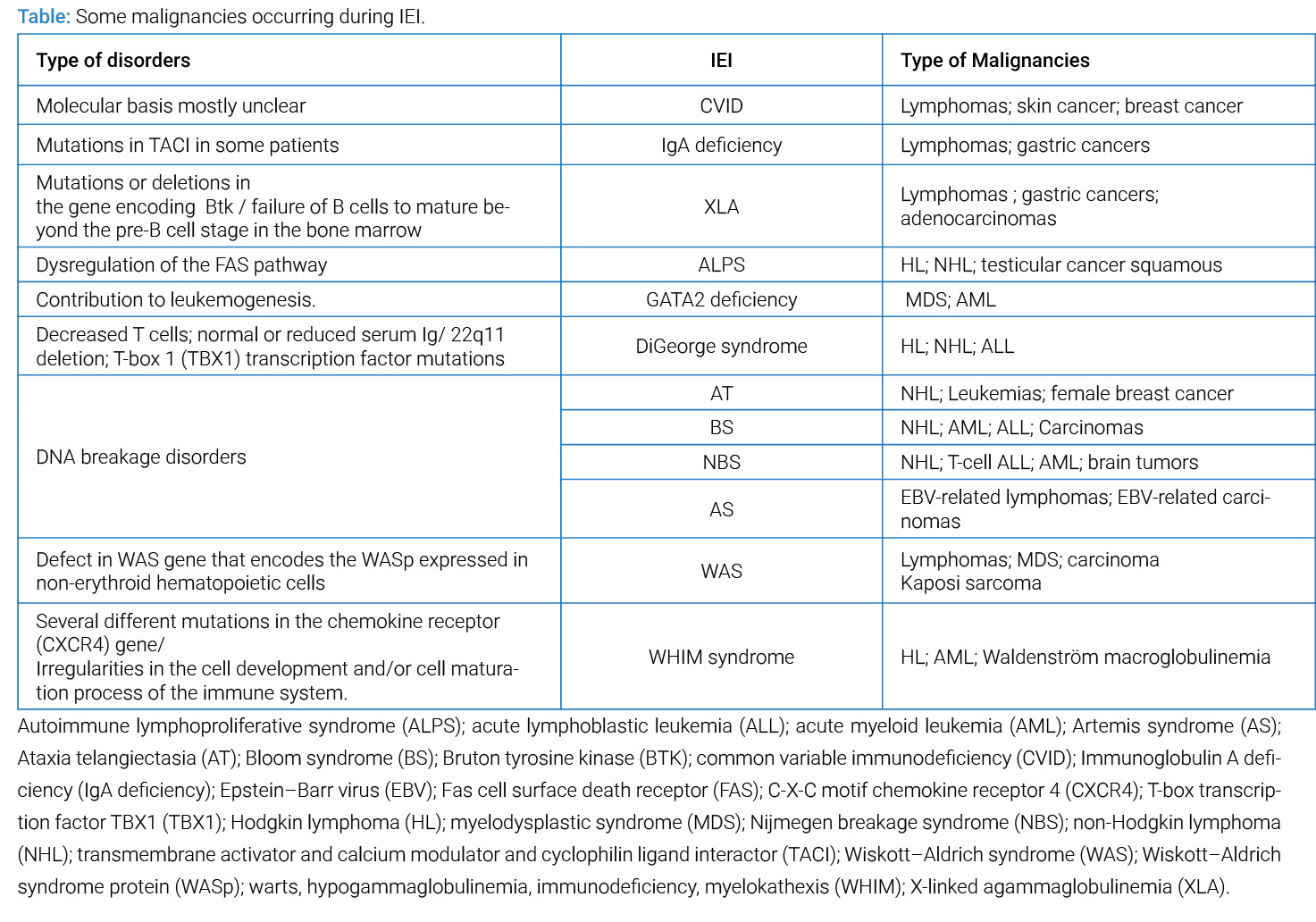
2. What IEI are complicated by malignancies and what types of malignancies complicate them (Table):
The type of malignancy that is seen is highly dependent on the specific IEI, the age of the patient, and probably the viral infection status, indicating that different pathogenic mechanisms may be implicated in each case [3,13,19–22].
Malignancies generally appear at earlier ages and in boys [23]. Lymphomas are the most frequently encountered tumor pathology in IEI [24,25]. These are mainly large B-cell NHL, with a high grade of malignancy, and EBV-induced lymphoproliferative diseases [6,7,13]. EBV is thus involved in 30% to 60% of lymphoma cases associated with IEI [26]. However, lymphoma can also reveal an underlying IEI. For example, in CVID, lymphoma develops before the onset of PID in 22% of cases and precedes the diagnosis up to several months [27]. Various studies have reported a several-fold increase in the incidence of lymphomas in IEI [24,25]. This particularity of immunodeficiency (including IEI) in favoring the development of lymphomas prompted the WHO to review the general classification of lymphomas and introduce a new category, which now groups these lesions under the overarching category of lymphoid proliferations and lymphomas associated with Immunodeficiency and Dysregulation (IDD-LPDs), acknowledging both deficiency and dysregulation of the immune system as underlying etiologies [28].
Gastric adenocarcinoma, thymoma, and rarely, melanoma, breast cancer, neuroblasto ma, medulloblastoma, liver, biliary tree and pancreas tumors represent some of other types of cancer with an increased relative risk in patients with IEI [24,29–31]. No malignancy was reported in patients with complement deficiency, phagocyte disorders and autoinflammatory diseases [12].
3. Clinico-biological and epidemiological particularities of Malignancies associated with IEI:
The clinico-biological presentation of the malignancies that appear in IEI presents some particularities from the histological and epidemiological points of view. There is 1.42-fold relative increased risk of cancer in subjects with IEI compared with age-adjusted surveillance [25]. Malignancies in IEI children and adolescents appear at a younger age and predominate in males [23]. Diffuse large B-cell type lymphomas of the extranodal infiltrations type predominates in younger age patients [32]. As in other publications [6,13,33,34], predominance of extranodal sites, rapid clinical progression, polymorphic cell population, diffuse large cell histology with B-cell origin, and EBV association were reported. On the other hand, patients with IEI and lymphoma have significant morbidity and mortality risks [35]. Another particularity in IEI-associated malignancies is that several IEI-related genes have been found to be somatically mutated [36].
Overall survival (OS) is less favorable in IEI patients experiencing malignancies; this fact could be related to the advanced disease stage, delayed admission time to the specialized centers, increased infectious comorbidities, and severe side effects following cytotoxic cancer therapies [13,37].
In their meta-analysis on behalf of the European Society for Immunodeficiencies patient registry, Kindle et al. [2] reported that in 1.7% of cases the disease was revealed by a malignant pathology and that during follow-up 8.9% of patients developed such pathology. As IEI is associated with malignancy occurrence, primary antibody deficiencies predominated in both cases. Tavakol et al. [12] also found that CVID represents the IEI most complicated by malignant transformations.
4. Recent advances in the research and treatment of malignancies associated with IEI:
Because of the high clinical variability and genetic heterogeneity for most IEI, high-throughput sequencing methods or Next-Generation Sequencing (NGS) are recommended [36]. Panel sequencing enables rapid, high-throughput analysis of multiple genes to increase the sensitivity of molecular diagnostics and simplify decision-making processes for IEI with high heterogeneity [38].
Several gene therapy clinical trials are currently running for many IEI [36]. On another level, for the context of gene therapy or gene editing approaches for IEI, strategies are needed to allow patients affected by ultra-rare conditions to benefit from cutting-edge technological advancements in therapeutics [39].
Autologous Haematopoietic Stem Cell Gene Therapy (HSC GT) has the potential to correct genetic defects across haematopoietic lineages without the complications of an allogeneic approach. HSC GT for IEI has been in development for the last two decades, and the first licensed HSC GT product for adenosine deaminase-deficient severe combined immunodeficiency (ADA-SCID) is now available [40].
However, oriented regulation of specific pathways through Monoclonal Antibodies (mAb), cytokines, and other drugs has now become central to the treatment of some related IEI manifestations as malignancies [36].
5. Practical recommendations for the management of these patients:
In general, once IEIs are diagnosed, physical exams as surveillance, with or without laboratory testing and imaging evaluations, are encouraged. Most importantly, patients should be informed to have a high index of suspicion for malignancies and report changes in their health. Education of physicians about the risk of malignancies during childhood in IEI and the awareness of considering underlying IEI in children who present with a malignancy will accelerate diagnosis, personalize treatment, and ultimately improve outcomes in the future [5].
Recent findings in IEI are increasingly convincing medical specialists in other fields that IEI may be at the basis of several major medical conditions, and the interest in defining the genetic etiology is growing [36]. Therefore, during the evaluation of malignancies in IEI, a multidisciplinary approach will be undoubtedly needed to differentiate nonmalignant and malignant lesions [13]. Additionally, in the setting of the lymphoproliferative process, the diagnosis of lymphoma and classification were more complicated and not always harmonious among histopathologists [41]. To avoid these discrepancies, collaboration among clinicians and histopathologists will be beneficial for accurate diagnosis [27]. Thus, the WHO classification of lymphomas [28], which incorporates a new category of lymphoproliferations and lymphomas associated with immunodeficiency, will facilitate the diagnosis and classification of such malignancies.
The most efficient treatment should provide a positive balance for immune protection in normal cells, while killing more malignant cells. Especially, patients with DNA repair defects should not receive radiomimetic agents [42]. Modified chemotherapy protocols with shorter duration or associated with rituximab, in the case of B-cell lymphomas, may be more beneficial with a favorable outcome and less toxicity [13]. Although IEI has always been linked to an increased susceptibility to cancer, there are specific defects, including, for instance, AT and XLA, that can present primarily with early forms of cancer, most often with lymphoma and leukemia [43,44].
Haematopoietic Stem Cell Transplant (HSCT) with reduced-intensity conditioning seems to be more effective in several disorders with improved post-HSCT survival [45]. Gene-editing procedures provided the proof of concept that gene therapy can be considered to cure IEI, especially in patients without HLA-matched stem cell donors in whom the toxicity of allogeneic procedures is high [35].
Conclusion
IEI are syndromes associating several conditions, including infections, chronic inflammations, autoimmune diseases, and malignancies. This malignant transformation is highly attributed to a lack of clearance of oncogenic viruses, a chronic inflammatory state, or a tumor escape phenomenon due to a lack of surveillance by the immune system.
These malignancies, which are the second most common cause of death after infections, appear during the course of certain IEI and are characterized by an early onset, a high degree of malignancy, and a more frequent fatal outcome than in patients without IEI. Lymphomas represent the most common type of malignancy, with specific histological features and more frequent involvement of EBV.
In addition to the usual diagnostic methods (Ig dosage, lymphocyte phenotyping, etc.), new molecular biology techniques are making a fundamental contribution to the diagnosis of these complex pathologies with a strong genetic background. These include high-throughput sequencing methods or NGS. Several gene therapy clinical trials are currently running for many IEIs. The most promising seems to be the Autologous HSC GT, which has the potential to correct genetic defects across haematopoietic lineages without the complications of an allogeneic approach.
Management of these patients requires follow-up in specialized centers, where diagnosis and rigorous monitoring can be carried out. Clinicians and biologists need to work together to diagnose malignant transformation as early as possible.
