Abstract
Poorly differentiated Pancreatic Neuroendocrine Carcinoma (pNEC) is a rare but highly aggressive neoplasm. The median survival is less than 12 months. We present the case of a 66-year-old man, incidentally diagnosed with pNEC during evaluation for a bilateral pulmonary embolism. He underwent distal pancreatectomy with splenectomy. After postoperative complications, pathological analysis confirmed high-grade pNEC. The patient received adjuvant radiotherapy for positive surgical margins. Six cycles of adjuvant chemotherapy with carboplatin–etoposide followed. This approach achieved a disease-free interval of 33 months. After developing an exclusive hepatic recurrence, the patient received several lines of sequential chemotherapy: capecitabine–temozolomide, capecitabine plus irinotecan, and Docetaxel. He reached an exceptional overall survival of more than 48 months, far exceeding the expected median for this condition. This case highlights the importance of multidisciplinary management and individualized sequential therapies. The distinctive outcome further suggests potential molecular or biological tumor characteristics may impact prognosis and therapeutic response.
Introduction
Pancreatic neuroendocrine carcinoma (pNEC) represents a rare but clinically relevant entity within the spectrum of pancreatic neuroendocrine tumors (pNETs). The estimated annual incidence is between 2.5 and 5 cases per 100,000 individuals [1]. Unlike well-differentiated Neuroendocrine Tumors (NETs), pNECs are high-grade, poorly differentiated neoplasms with aggressive biological behavior, similar in presentation and progression to large or small cell neuroendocrine carcinomas of the lungs [1,2]. Histopathologically, pNECs are characterized by a high proliferation rate (Ki-67 index >20%, typically >55%) and atypical cellular morphology, which clearly distinguishes them from well-differentiated NET tumors [3,4]. Most cases are diagnosed at advanced stages, often with hepatic and lymph node metastases, limiting the potential for curative surgical intervention. Up to 60% of patients present with metastatic disease at the time of diagnosis, significantly limiting the potential for curative surgical intervention [2]. However, several studies have demonstrated that palliative resection of the primary tumor is associated with improved prognosis, with a median survival of 12 months compared to 8 months in patients who do not undergo surgery [5]. Furthermore, combining surgery with adjuvant chemotherapy or radiotherapy can increase median survival to up to 19 months [5].
Diagnosis of pNEC requires a combination of functional imaging techniques (such as 68Ga-DOTATATE positron emission tomography/computed tomography (PET/CT) or Fluorodeoxyglucose (FDG) PET/CT) and biopsy with immunohistochemistry (including markers such as chromogranin A, synaptophysin, and Ki-67 index (Ki-67)) [5,6]. Due to the high aggressiveness of pNEC, treatment regimens are similar to those for small-cell lung carcinoma, typically involving platinum-etoposide chemotherapy. However, response rates and long-term survival remain limited. The prognosis for patients with pNEC is poor, with median overall survival rarely exceeding 12 months in advanced stages [8].
Case Presentation
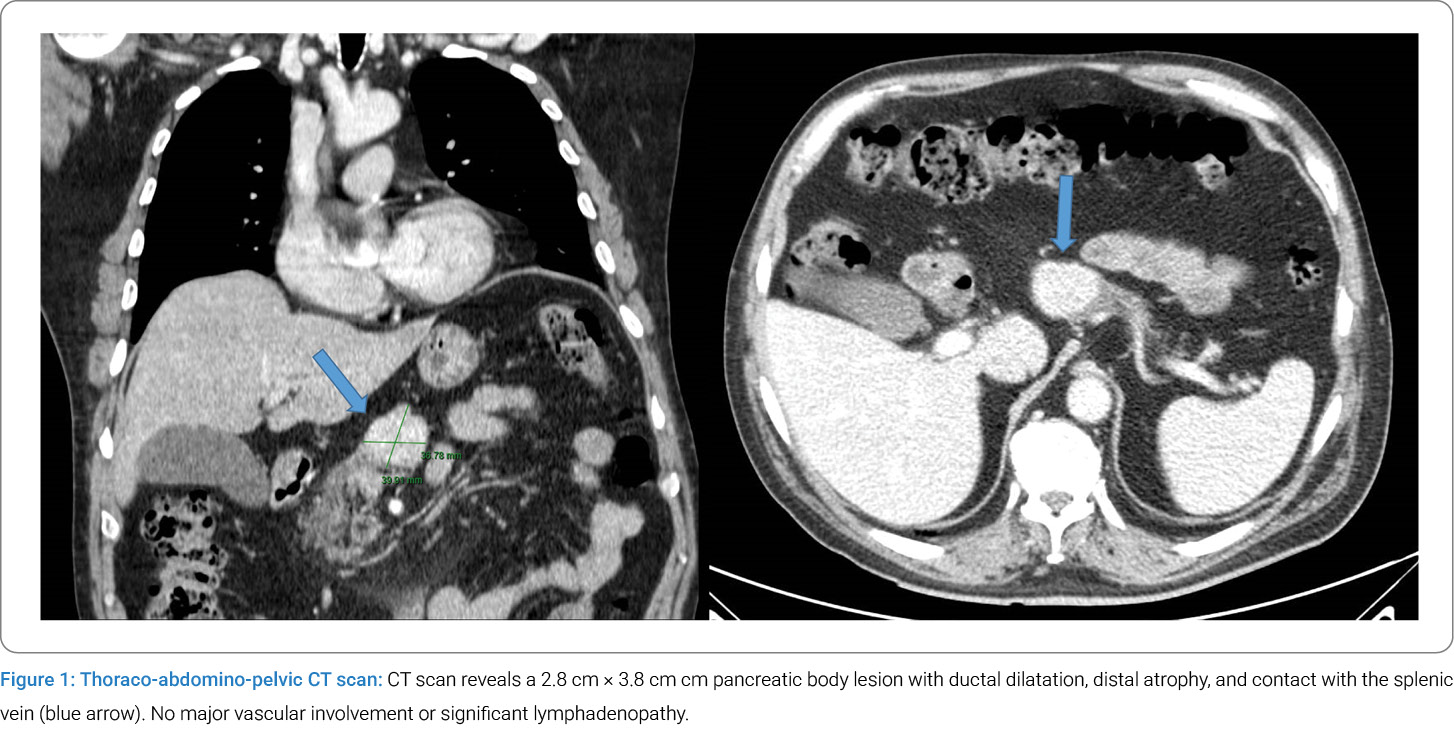
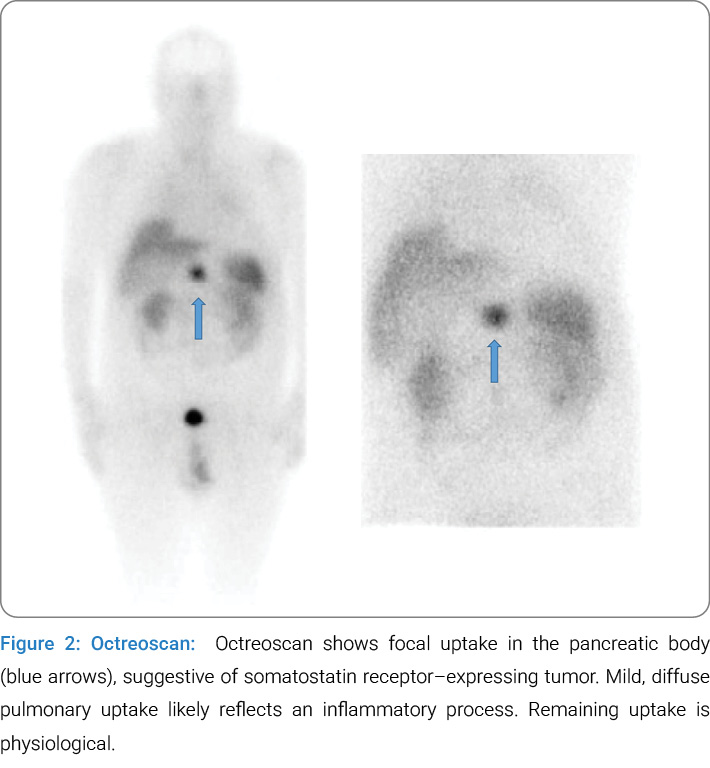
We present the case of a 66-year-old man, a former smoker (23 pack-years), with a history of type 2 diabetes and grade 2 obesity. He was admitted in 2021 to the internal medicine department for pneumonia associated with SARS-CoV-2 infection. During hospitalization, he was incidentally diagnosed with bilateral pulmonary embolism. A malignancy work-up was initiated, including colonoscopy, which revealed polyps and hemorrhoids. A whole-body CT scan showed a pancreatic mass in the body of the pancreas, infiltrating the splenic vein but without lymph node involvement (Figure 1). An endoscopic ultrasound revealed a heterogeneous hypoechoic mass with ill-defined borders, measuring 39 mm × 37 mm, with infiltration of the splenic vein. Fine needle aspiration suggested a well-differentiated neuroendocrine tumor. This initial diagnosis was later revised based on the definitive pathology of the surgical specimen, highlighting diagnostic uncertainty and the evolving nature of tumor classification. An Octreoscan showed a mass in the body of the pancreas with somatostatin receptor expression (Figure 2). The case was discussed at a multidisciplinary tumor board, and surgical intervention was recommended. A distal pancreatectomy with splenectomy was performed on February 18, 2021, followed by multiple postoperative complications: extensive thrombosis in the left lower limb, postoperative anemia, and several intra-abdominal hematomas. Additionally, the patient developed a biliopancreatic fistula and multiple fluid collections at the surgical site. Percutaneous drainage was performed, with negative microbiological cultures, and the patient was treated with broad-spectrum antibiotics. An endoscopy with ERCP (Endoscopic retrograde cholangiopancreatography) revealed extrinsic gastric compression and stenosis of the common bile duct, for which a plastic stent was placed. The patient was discharged with home hospitalization, antibiotics, and follow-up.
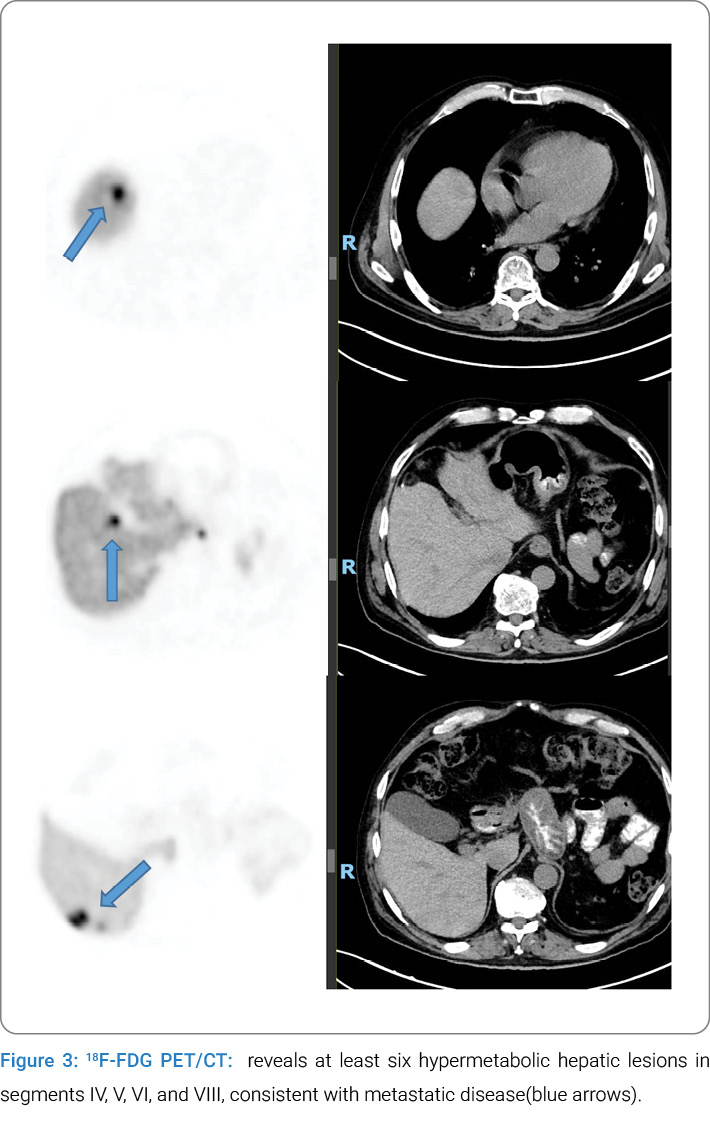
The pathological analysis of the surgical specimen revealed a poorly differentiated pNEC, intermediate grade according to the 2017 WHO classification (PanNETs/PanNECs), with pathological staging of pT2 pN1 and affected margins. Ki-67: 55%. The patient completed six cycles of adjuvant chemotherapy with carboplatin (AUC 5 IV on day 1 and etoposide 100 mg/m² IV on days 1–3 every 3 weeks), followed by adjuvant radiotherapy due to the presence of microscopically involved surgical margins. The patient remained in complete remission until November 2023 (33 months of recurrence-free interval), when 18F-FDG PET/CT and biopsy (with a Ki-67 index of 50%) confirmed exclusive hepatic recurrence (12 lesions, all in the right hepatic lobe, Figure 3). At that time, a 68Ga-DOTATATE PET/CT scan was also performed, which showed no pathological uptake at any level, including the hepatic lesions. Three additional cycles of carboplatin and etoposide were administered. Surgical intervention was considered but ultimately contraindicated due to the presence of esophageal varices and evidence of tumor progression on Magnetic Resonance Imaging (MRI). A new chemotherapy regimen with capecitabine and temozolomide was initiated. After eight cycles, hepatic disease progression was observed, prompting the initiation of third-line therapy with biweekly XELIRI (oral capecitabine 1000 mg/m2 bid 1 day–14 days plus Irinotecan 180 mg/m2 iv every 3 weeks) for five cycles. Upon further progression, enrollment in a clinical trial was considered; however, the patient was not included due to the unavailability of open slots.
Finally, a fourth-line treatment with docetaxel (75 mg/m2 every 3 weeks) was initiated, and the patient has remained with survival exceeding 48 months since diagnosis.
Discussion
Poorly differentiated pNEC is a rare but highly aggressive tumor, accounting for less than 1% of pancreatic neoplasms. At diagnosis, up to 70% of patients present with metastatic disease, most commonly to the liver (80%), followed by bone and lung involvement [1,2]. Morphologically and clinically, pNEC closely resembles small cell lung carcinoma [1,2]. Median survival rarely exceeds 12 months despite chemotherapy, and is limited to 4 months–6 months in the absence of treatment [5], highlighting the notable contrast with the clinical course observed in our case.
Our patient, a 66-year-old man with multiple comorbidities, was incidentally diagnosed with a pNEC during an evaluation for occult malignancy prompted by bilateral pulmonary embolism. The tumor, located in the body of the pancreas and demonstrating somatostatin receptor expression, initially suggested a well-differentiated NET. However, the definitive diagnosis of poorly differentiated large-cell neuroendocrine carcinoma (pNEC) was established following surgical resection. Favorable prognostic factors in this case included [5]; resection of the primary tumor, somatostatin receptor overexpression, and an Eastern Cooperative Oncology Group (ECOG) performance status of 0. Emerging evidence indicates that multimodal therapeutic strategies, including surgery and radiotherapy as applied in this case, can improve clinical outcomes. This observation is supported by reports from the 2000s, which demonstrated that patients undergoing chemotherapy followed by primary tumor resection achieved improved Progression-free survival (PFS) [5].
Additionally, retrospective analyses suggest that palliative resection of the primary tumor or the use of radiotherapy may improve survival in patients with metastatic pNEC. Jiang et al. reported that resection of the primary tumor, combined with chemotherapy, was associated with improved survival in non-functional pancreatic NECs, with a median survival of 15 months following surgery compared to 5 months without surgical intervention, irrespective of chemotherapy administration [6].
Feng et al. reported that among 350 patients, the 50 individuals (14.3%) who underwent surgery—either with or without metastasectomy—combined with chemotherapy had a median overall survival of 12 months, compared to 8 months in those who did not undergo surgery [5]. Additionally, male sex and a Ki-67 index greater than 55% have been identified as factors associated with poorer prognosis [7]. Therefore, in our patient, the combination of being male and having a Ki-67 index of less than 55% justifies his better clinical course.
pNEC is detectable on FDG-PET scans, with a high standardized uptake value, and is usually negative or has focal avidity on SSRS [8]. 18F-FDG PET, It should be performed in the case of a negative or slightly positive 68Ga-DOTA-peptides PET scan for assessing the dedifferentiation status, to guide a correct therapeutic strategy, and to evaluate the prognosis. The approach of combined receptor and metabolic imaging can improve diagnostic accuracy, especially considering the heterogeneity of these lesions. Therefore, 68Ga-DOTA-peptides and 18F-FDG PET should be considered complementary in patients with GEP-NENs [9].
Our patient initially demonstrated uptake of the primary tumor on an Octreoscan, suggesting Somatostatin Receptor (SSR) expression. In contrast, the hepatic metastatic progression showed no SSR expression on the 68Ga-DOTATATE PET/CT scan. This loss of SSR expression, together with the marked rise in proliferative activity, supports a transformation toward a more aggressive tumor phenotype. These findings underscore the importance of reassessing both the Ki-67 index and SSR expression in recurrent or metastatic disease, as such biological shifts may have significant prognostic and therapeutic implications. Wang et al. [10] reported that Ki-67 variability occurred in 53.3% of patients with gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs), with 40% showing up regulation of Ki-67 during the disease course. This increase was associated with significantly shorter overall survival and was identified as an independent prognostic factor. The absence of genomic data (e.g., p53 status, RB1, or microsatellite instability) represents a limitation, especially in cases with atypical clinical progression, where the molecular profile could provide prognostic or therapeutic insight.
Historically, chemotherapy regimens based on cisplatin and etoposide, extrapolated from the treatment of small-cell lung carcinoma, were employed [11,12]. However, retrospective studies such as the Nordic NEC trial have demonstrated that carboplatin provides comparable efficacy with a more favorable toxicity profile, particularly regarding renal toxicity [13]. Based on this evidence, our patient received six cycles of carboplatin and etoposide, followed by adjuvant radiotherapy due to microscopically involved surgical margins. The patient exhibited excellent tolerance to this first-line treatment, maintaining an ECOG performance status of 0, and achieved a disease-free interval of 33 months (compared to a reported median of 12 months). Upon isolated hepatic recurrence and considering the favorable prior clinical course, three additional cycles of carboplatin–etoposide were administered. Surgical intervention was contemplated but ultimately abandoned due to the presence of esophageal varices and tumor progression observed on MRI. Subsequently, second-line chemotherapy with capecitabine and temozolomide was initiated. In the first-line palliative setting, prior use of carboplatin and etoposide as part of adjuvant therapy may contribute to poorer outcomes, with a reported PFS of approximately 2.5 months to 3 months [14].
The second-line treatment with capecitabine and temozolomide was selected based on its reported PFS of up to 5.4 months, which compares favorably to alternative regimens such as FOLFIRI (Leucovorin, fluorouracil, and irinotecan) or FOLFOX [15] (Leucovorin, fluorouracil and oxiplatin). However, disease progression was observed after 8 cycles, prompting the initiation of third-line therapy with XELIRI, which similarly resulted in progression after 5 cycles. Notably, the disease-free intervals following these two lines were shorter than those observed with prior treatments. Subsequently, fourth-line therapy with docetaxel was introduced, achieving disease stabilization after six cycles (notably, the literature reports that in this type of tumor, PFS is typically less than 3 months) [16]. Despite these challenges, the patient has sustained an overall survival exceeding 48 months since diagnosis, significantly surpassing the typical survival expectations for poorly differentiated pNEC. This case underscores the value of a personalized, sequential therapeutic strategy that integrates surgery, chemotherapy, radiotherapy, and multidisciplinary management to optimize outcomes in this aggressive malignancy.
In light of these therapeutic challenges and outcomes, cabozantinib has emerged as a promising option for patients with Pancreatic Neuroendocrine Tumors (pNETs) who have progressed following multiple lines of therapy. The Phase III CABONEN trial [17], presented at ESMO 2024 congress, demonstrated a significant improvement in PFS (11.4 vs. 3.0 months; HR 0.27), highlighting its efficacy. Its mechanism of action, involving multikinase inhibition of MET, VEGFR, and AXL, supports its utility in refractory pNETs by targeting multiple signaling pathways critical to tumor progression.
Given the patient’s Ki-67 index of 55% (i.e., <60%), we plan to initiate cabozantinib as a fourth-line palliative treatment upon progression of the current regimen.
Throughout treatment, the patient has maintained an ECOG performance status of 0 despite multiple therapeutic lines, reflecting preserved quality of life, which supports the rationale for continuing palliative therapy.
Conclusion
This case report describes an exceptional outcome in a patient with poorly differentiated pNEC. The patient achieved overall survival exceeding 48 months, despite the typically aggressive nature of this disease. Most patients have a median survival of less than 12 months. This prolonged survival underscores the critical role of a tailored, multidisciplinary approach. Such an approach involves surgical resection, adjuvant chemoradiotherapy, and sequential systemic therapies to manage high-grade neoplasms. The patient’s atypical clinical course suggests potential heterogeneity within pNEC. This may be driven by distinct biological or molecular features that need further investigation. These findings highlight the need for personalized therapeutic strategies in pNEC. They also emphasize the importance of prospective studies to identify prognostic biomarkers and optimize treatments. Ultimately, this may improve outcomes for patients with this challenging malignancy.
Conflict of Interest
Luis Cabezón-Gutiérrez reports he received payment for presentations of Roche, AstraZeneca, Bristol Myers Squibb, Merck Serono, Ipsen Pharma, Grunenthal, Kyowa Kirin, Pfizer, and Eisai, and received support for attending meetings from Roche and Merck. Eli Lilly, Bristol-Myers Squibb, and Nutricia. Vilma Pacheco Barcia reports she received a grant as an award from Merck and FSEOM and a grant from Pfizer. Payment for presentations of Merck, Eli Lilly, Eisai, and Pierre Fabre, and received support for attending meetings from Roche, Eli Lilly, Bristol-Myers Squibb, Merck, Amgen, Merck Sharp and Dohme, and Nutricia. Vilma Pacheco Barcia also reports she participated in an advisory board from Advanced Accelerator Applications, a Novartis company, and Nutricia. Sara Custodio-Cabello has received honoraria (outside of this submitted study) from Fresenius, Astellas Pharma, Merck, and Abbott, and received support for attending meetings from Pierre-Fabre and Amgen. Magda Palka-Kotlowska has received payment for presentations of Pfizer, Devon, Pharmamar, and Esteve, and received support for attending meetings from Pfizer and Novartis. José Ramón Sevilla-Resúa, Sheherezade Gallego-Nieto, Irene Hidalgo Hernandez, and Beatriz Chacón-Ovejero have no conflicts of interest to declare. All the authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Cite this article
Sevilla-Resúa JR, Pacheco-Barcia V, Custodio-Cabello S, Palka-Kotlowska M, Gallego-Nieto S, Hernandez IH, et al. Long-Term Survival in Poorly Differentiated Pancreatic Neuroendocrine Carcinoma: A Multimodal Case Study. Clin Oncol J. 2025;7(1):1–6.
