Quality of Long-Term Remissions in Patients with Relapsed Hodgkin Lymphoma after Autologous Stem Cell Transplantation
* Metzner B;
Muller TH;
Casper C;
Kimmich C;
Petershofen EK;
Thole R;
Voss A;
Kohne CH;
-
* Metzner B: Department of Oncology and Haematology, Klinikum Oldenburg, Oldenburg, Germany
-
Muller TH: Red Cross Blood Transfusion Service NSTOB, Oldenburg, Germany
-
Casper C: Department of Oncology and Haematology, Klinikum Oldenburg, Oldenburg, Germany
-
Kimmich C: Department of Oncology and Haematology, Klinikum Oldenburg, Oldenburg, Germany
-
Petershofen EK: Red Cross Blood Transfusion Service NSTOB, Oldenburg, Germany
-
Thole R: Department of Oncology and Haematology, Klinikum Oldenburg, Oldenburg, Germany
-
Voss A: Department of Oncology and Haematology, Klinikum Oldenburg, Oldenburg, Germany
-
Kohne CH: Department of Oncology and Haematology, Klinikum Oldenburg, Oldenburg, Germany
Novel Findings and Clinical Impact
1. What is the new aspect of our work?
Long-term remissions after autologous stem cell transplantation (ASCT) in patients with relapsed Hodgkin lymphoma are observed relatively frequently. The quality of life after such remission has been rarely addressed especially in patients followed for up to 30 years. The data presented here contain such details.
2. What is the central finding of our work?
The vast majority of patients with long-term remission have a very good or favorable performance status. Secondary malignancies are relatively frequent.
3. What is (or could be) the specific clinical relevance of our work?
These findings may be essential for counselling patients on their treatment options and to motivate them to undergo regular cancer screening post-transplantation.
Abstract
Background: The optimal therapy for patients with relapsed Hodgkin lymphoma remains controversial. In this context, the quality of long-term remissions after high-dose therapy and Autologous Stem Cell Transplantation (ASCT) is of special interest, but remains insufficiently studied.
Case Presentation: To evaluate long-term outcomes, we regularly monitored 73 patients with relapsed Hodgkin lymphoma for up to 30 years after ASCT in our outpatient department.
Results: Long-term remissions were observed frequently, with a 10-year Progression-free survival (PFS) of 59% and a 10-year Overall Survival (OS) of 62%. Notably, 55% of long-term survivors had an excellent performance status (ECOG 0) while 42% had mild complaints (ECOG 1), mostly attributed to age-related conditions. The one-year non-relapse mortality was low (1/73, 1.4%). However, secondary invasive malignancies were relatively common, affecting 10 patients within 2 years–19 years post-ASCT. Multivariate analysis of OS and PFS identified the age and the relapse type (early relapse before ASCT within <12 months from end of induction therapy vs. late relapse) as significant prognostic factors. Patients with advanced age and early relapses had a more unfavorable course.
Conclusions: ASCT is an effective treatment for relapsed Hodgkin lymphoma, offering high rates of long-term remission with favorable performance status. However, given the risk of secondary malignancies, systematic lifelong cancer screening should be considered for these patients.
Abbreviations: High-Dose Therapy (HDT); Progression-free survival (PFS); Overall survival (OS); Hazard ratio (HR); Confidence interval (CI)
Introduction
High-Dose Therapy (HDT) with Autologous Stem Cell Transplantation (ASCT) is a well-established and effective treatment for lymphoma patients, including those with relapsed Hodgkin lymphoma, offering a significant proportion of long-term remissions [1–12]. However, a considerable number of patients relapse after ASCT. With the advent of new therapeutic strategies, the optimal treatment approach remains a topic of ongoing discussions [13,14]. In this context, the quality of long-term remissions and the long-term toxicity of ASCT warrant closer examination. Specifically, assessing the quality of remission in terms of performance status (ECOG score), non-relapse mortality, and the incidence of secondary malignancies is essential. To address this gap, we analysed data from patients with relapsed Hodgkin lymphoma treated with ASCT at our institution between 1994 and 2020, with a particular focus on the quality of remission [15].
Case Presentation
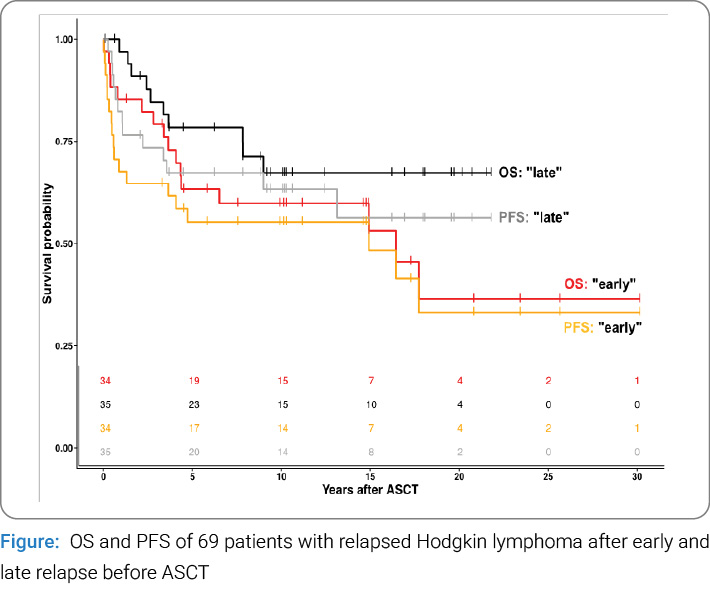
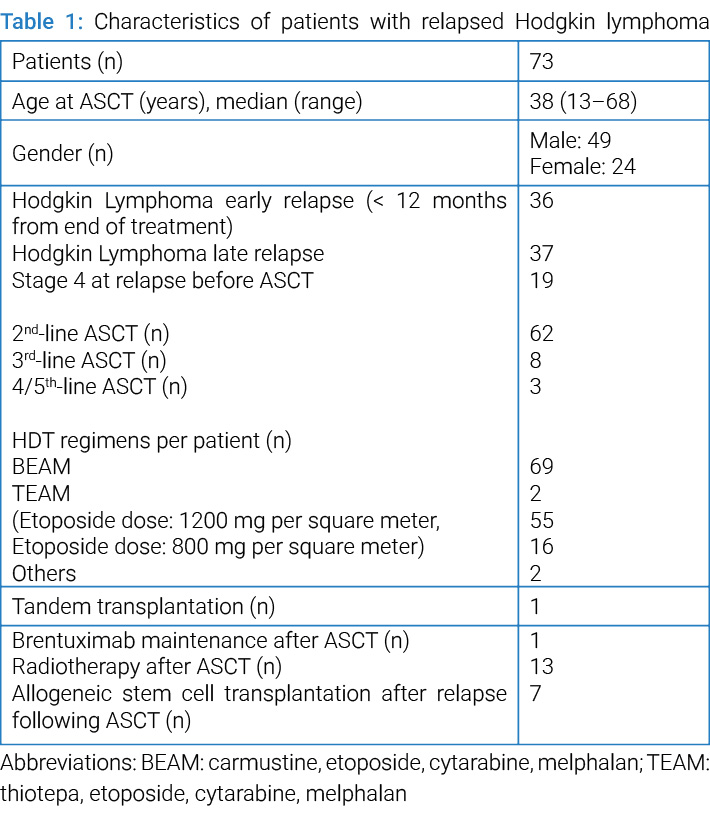
During the study period between 1994 and May 2020, 73 consecutive patients with relapsed Hodgkin lymphoma were treated with HDT and ASCT in our institution, which is accredited by the Joint Accreditation Committee ISCT Europe (JACIE) of the European Society for Blood and Marrow Transplantation (EBMT). In every case, the diagnosis was confirmed by a reference pathologist with special experience in malignant lymphomas. Most patients were controlled after ASCT in our outpatient department; only a smaller part of the patients got follow-up by an oncologist close to home (Figure). The clinical data of the patients were analysed, especially regarding the performance status, the NRM and the occurrence of secondary malignancies. The characteristics of these 73 patients are shown in Table 1. One patient received two HDT courses (as tandem transplantation within a maximum of six months after the first transplantation). Stem cell apheresis and cryopreservation, as well as the analysis of CD34+ cells of peripheral blood and stem cell products, were performed in the blood bank of the German Red Cross Transfusion Service NSTOB near our hospital. After hospital discharge following HDT and ASCT, the patients were controlled every 4 weeks–12 weeks in the first year after ASCT and every 3 months–6 months in the 2nd year after ASCT, every 6 months from the third until the fifth year and every 12 months afterwards. The HDT regimens that were mostly used within or according to multicentric clinical trials are shown in Table 1. Most patients received the BEAM regimen (with BCNU, etoposide, cytarabine and melphalan) with two distinct variations. The patients were treated with etoposide in a dose of either 800 mg or 1200 mg per square meter body surface according to the protocol of a German study [16–18]. The stem cell products always consisted of at least 2.0 million CD34+ cells per kilogram body weight. The following drugs were used prophylactically: acyclovir 400 mg two times daily orally as prophylaxis against herpes simplex infection, in the case of mucositis intravenously 250 mg three times daily, as infection prophylaxis, additionally ciprofloxacin, fluconazole, amphotericin B suspension and inhalation with pentamidine until bone marrow regeneration, after regeneration, cotrimoxazole for three months after ASCT. Granulocyte colony-stimulating factor (G-CSF) was used from day one after autologous stem cell reinfusion until bone marrow regeneration, usually for ten days. The salvage chemotherapy before ASCT consisted of the DHAP regimen (usually two cycles with dexamethasone, high-dose cytarabine and cisplatin [16–18], n=50) or the Dexa-BEAM regimen (usually two cycles with dexamethasone, BCNU (carmustine), etoposide, cytarabine and melphalan [19], n=8) or other regimens (n=4). Seven patients received an allogeneic stem cell transplantation after relapse following ASCT. They were censored at the allogeneic transplantation date. Excluded from the analysis were three patients who had been treated with ASCT in the fourth or fifth therapy line and one patient with an alternate HDT regimen without etoposide.
Statistics: All statistical analyses were conducted in R statistical software version 4.3.3 and R Studio version 2024.12. Time-to-event data, including Overall Survival (OS) assessed as time from ASCT to death from any cause) and Progression-free survival (PFS) time from ASCT to either relapse or death from any cause), were analysed using Kaplan-Meier (KM) estimators. Survival curves were generated with the survival and survminer packages.
For univariate and multivariate survival analyses, a robust version of the Cox proportional hazards model was applied using the coxrobust package. Hazard Ratios (HR) and 95% Confidence Intervals (CI) were reported for all Cox regression analyses. All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant. Excluded from the analysis were three patients who had been treated with ASCT in the fourth or fifth therapy line and one patient with an alternate HDT regimen without etoposide. These three patients had died due to relapsed lymphoma, a secondary invasive malignancy (NSCLC), or a brain haemorrhage (see NRM). The fourth patient also died (due to relapse and subsequent allogeneic transplantation). Data were analysed as of 26th January 2025.
Results
The median follow-up for the 43 surviving patients was 10 years after ASCT, with a range of 0.1 year to 30 years. Among the 73 patients, 25 experienced a relapse between 0.1 year and 4.7 years post-ASCT (median: 0.5 years). No relapses were observed beyond 4.7 years following ASCT. Six patients were lost to follow-up, including one who was lost after one month due to follow-up abroad, while the remaining five were lost later in the course of follow-up. The OS rates at five years and ten years were 70% and 62%, respectively. Fifteen-year and 20-year OS were 59% and 51%, respectively. The five-year and 10-year PFS were 60% and 59%, respectively. Fifteen-year and 20-year PFS were 52% and 44%, respectively. The median PFS was 17.7 years, whereas the median OS was not reached.
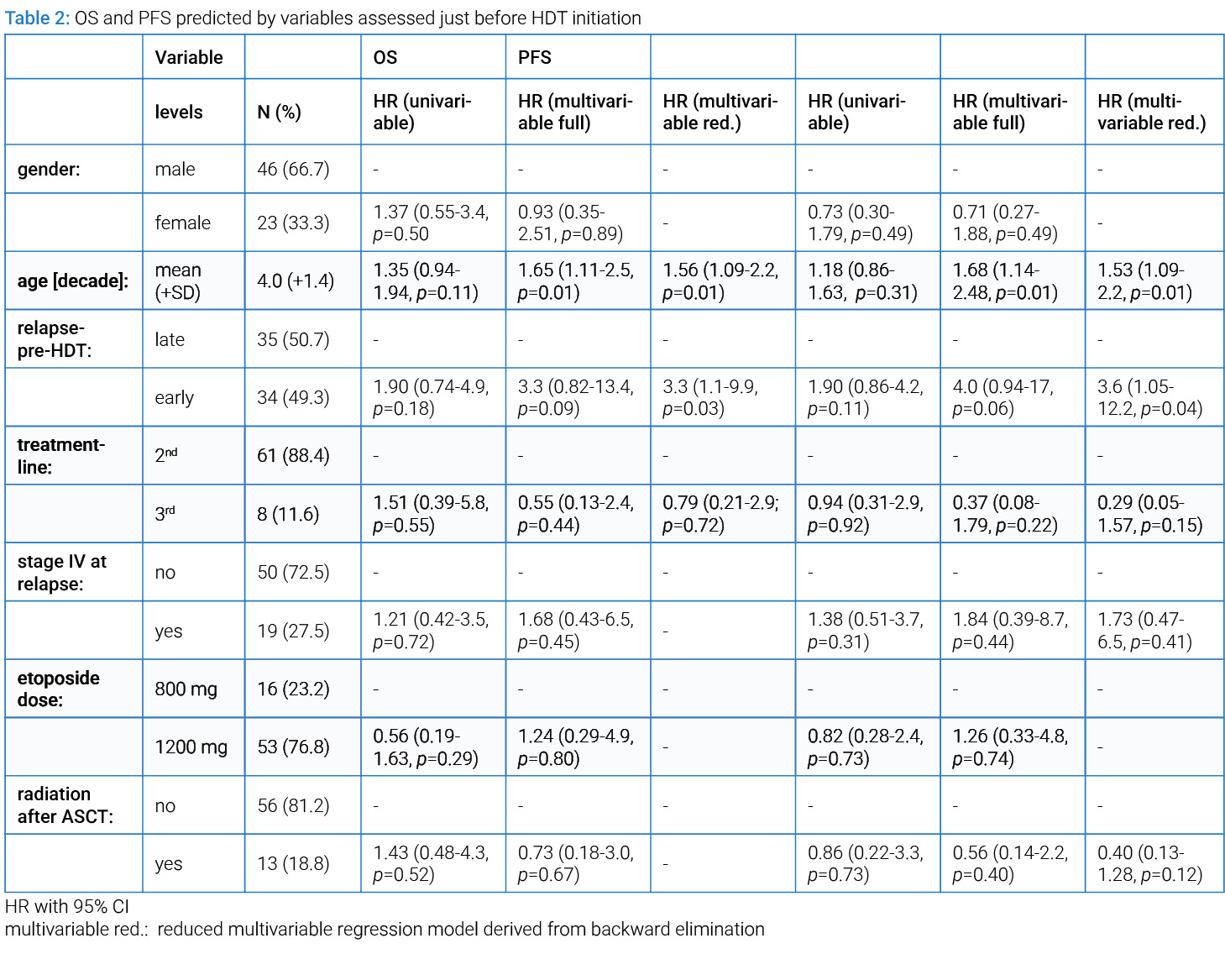
Prognostic factors: Multivariate analysis of PFS identified the age and the relapse type (early relapse before ASCT within <12 months from end of induction therapy vs. late relapse) as significant prognostic factors. Patients with advanced age and early relapses had a more unfavorable course. No further significant prognostic factors were identified regarding sex, Ann Arbor stage IV at relapse, etoposide dose 800 mg vs. 1200 mg in the BEAM regimen, or radiotherapy after ASCT (Table 2).
Performance status and complaints of patients with long-term remissions: Thirty-seven of 73 patients were evaluable for performance status (ECOG score) at last follow-up, as 30 patients had died and 6 patients were lost to follow-up. Among these, 21 patients (56.8%) had an ECOG score of 0, with 19 reporting no complaints and two experiencing minor polyneuropathy-related symptoms. Fifteen patients (40.5%) had an ECOG score of 1 due to conditions such as polyneuropathy (n=5), mild fatigue symptoms (n=3), degenerative spine disease (n=3), degenerative joint disease (n=2), post-zoster complaints (n=2), cardiac problems like coronary heart disease (n=1), peripheral artery occlusive disease (n=1), chronic obstructive lung disease (n=1), diabetes mellitus (n=1) and post-COVID-19 fatigue (n=1). One patient (2.7%) had an ECOG score of 3 because of cardiac and pulmonary problems (partly due to cigarette smoking) and polyneuropathy. All these symptoms were diagnosed after treatment.
Secondary invasive malignancies: Ten of 73 patients developed 13 secondary invasive malignancies: acute myeloid leukemia (n=2; 18 years and 19 years after ASCT, respectively), myelodysplastic syndrome (n=1; 3 years after ASCT), Burkitt lymphoma (n=1; 15 years after ASCT), mycosis fungoides (n=2; 5 years and 6.5 years after ASCT, respectively), non-small-cell lung cancer (n=1; 2.3 years after ASCT), bladder cancer (n=1; 6 years after ASCT), prostate cancer (n=1; 7 years after ASCT), rectal cancer (n=1; 6 years after ASCT), endometrial cancer (n=1; 19 years after ASCT), nasopharyngeal carcinoma (n=1; 2 years after ASCT), tongue cancer (n=1; 14 years after ASCT). Four of these 10 patients were alive at the last follow-up, as the secondary malignancy was not advanced in the two cases of mycosis fungoides, in the prostate cancer, and the endometrial cancer.
Non-relapse mortality: Nine patients died due to the following complications: acute myeloid leukemia (19 years after ASCT), advanced tongue cancer (15 years after ASCT), brain haemorrhage as complication of Immune Thrombocytopenia (ITP) (5 years after ASCT), an aggressive viral infection with multiorgan failure (3 years after ASCT), sepsis shortly after ASCT in one patient (2.6 weeks after ASCT) and unclear causes in three further patients (3 years, 4 years and 9 years after ASCT, respectively) which were lost to follow-up. One female patient developed pulmonary fibrosis (probably due to radiotherapy, bleomycin and BCNU before ASCT), underwent lung transplantation 14 years post-ASCT, and ultimately died at 18 years post-ASCT from complications related to immunosuppression, COVID-19 infection, leukoencephalopathy and secondary acute myeloid leukemia. The 1-year non-relapse mortality was 1/73 due to the mentioned sepsis before engraftment.
Discussion
Our data show a relatively high proportion of long-term remissions in patients with relapsed Hodgkin lymphoma after ASCT. The 5-year PFS is 61%, 10-year PFS 59%. The 5-year OS is 70%, the 10-year OS 62%. Our median follow-up was 10 years, maximum 30 years. For comparison: Epperla et al. [2] describe a 5-year PFS of 49% and a 5-year OS of 76%, Stamatoullas et al. [20] a 5-year PFS of 54% and a 5-year OS of 67%. Longer published observation times are rare, and most available studies have a shorter follow-up. Therefore, our results provide valuable insights.
A key finding of our analysis is the high quality of long-term remissions in patients with relapsed Hodgkin lymphoma after ASCT. Of the evaluable patients, 55% had an ECOG score of 0, while 42% had a favorable ECOG score of 1 with only mild, likely age-related complaints. Only 3% had an unfavorable ECOG score of 3. Comparable data in the literature are scarce, as long-term remission patients are typically followed-up by their general practitioners. However, this information is crucial for comparing treatment modalities and for patient counseling. Of interest is a publication of Mounier et al. [21] describing a high proportion (37%) of severe long-term fatigue in a cohort of 1671 different patients with non-Hodgkin lymphomas after diverse treatments. Smeland et al. [22] describe a cohort of 271 patients with diverse malignant lymphomas treated with ASCT (86% BEAM regimen). After a follow-up of eight years from ASCT they suffered with a relatively high proportion (30%) from grade 2 chronic fatigue. Georges et al. [23] published the results of 268 patients with different malignant lymphomas observed for 12 years (median) after ASCT. They observed a good performance score (Karnofsky ≥80) in 87% of these patients. Also interesting is the observation of Lemieux et al. [24] “that physical, social, and functional well-being are preserved” in 47 fit older patients (≥ 60 years old) following ASCT (after BEAM or BEAC) in patients with non-Hodgkin lymphoma. Minn et al. [25] summarise their analysis of 154 patients with refractory or relapsed Hodgkin lymphoma following ASCT that “overall quality of life did not differ from the general population, but ASCT survivors did note reduced functioning and some worse symptoms.” Ullrich et al. [26] analysed 553 patients with diverse diagnoses treated with ASCT. They found that 36% of non-myeloma patients suffered from high fatigue 11 years (range 4 years–20 years) after ASCT, clearly more than in our patient cohort. These heterogeneous findings regarding quality of life in long-term ASCT survivors highlight the need for standardized assessment tools. Moreover, they may reflect differences in patients´ and physicians´ expectations regarding post-ASCT recovery and well-being.
The outcome of ASCT in this patient cohort is relatively good as expected: 10-year OS 62% and PFS 59%. As the non-relapse mortality within one year is low (1/73), ASCT can be assessed as a treatment modality with high efficacy and low long-term toxicity. This should be considered for the choice of the treatment modality. The fact that we identified only two prognostic factors is probably caused by our small patient cohort and should not be overestimated as some further prognostic factors are known [9,12,16,17]. However, an ASCT in second remission should usually be preferred as for ASCT in third remission worse results were observed which were not statistically significant. A recent study by Metzner et al. [27] highlights the relatively high incidence of secondary malignancies and underscores the need for systematic lifelong cancer screening post-ASCT to improve patient outcomes. In this context, the following statement by Goodman et al. [28] is of special interest: “Survivors of ASCT had an elevated risk of secondary malignancies compared with the cancer risk in the general population, but when compared with patients with Hodgkin lymphoma in SEER (Surveillance, Epidemiology and End Results, a programme of the National Cancer Institute), the risk was less pronounced”. Additionally, some of the secondary malignancies are likely expected given the partly high patient age, and it is a known observation that patients having cancer once are predisposed to having more cancers.
The primary limitation of our study is the relatively small patient cohort which is inadequate for an in-depth analysis of prognostic factors. Additionally, we focussed solely on performance status and patient complaints without broader quality of life assessment. However, a strength of our study is the systematic long-term follow-up for up to 30 years by an experienced oncologist.
In conclusion, long-term remissions, particularly after second-line therapy, are common and frequently associated with good performance status. Given the relatively high frequency of secondary malignancies, systematic llifelong cancer screening should be considered following ASCT.
Acknowledgement
We thank Mona Temel for contributing to the collection of data.
Data availability: The datasets generated or analyzed during this study are available from the corresponding author on reasonable request.
Authorship: All authors met the four criteria for authorship (Substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data for the work; Drafting the work or revising it critically for important intellectual content; Final approval of the version to be published; Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved).
Ethics approval: The protocol was approved by the Medical Ethics Committee of the Carl von Ossietzky University Oldenburg and carried out in accordance with the Declaration of Helsinki.
Consent to participate: Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors declare that they have no conflicts of interest.
References
- Ansell SM. Hodgkin lymphoma: 2025 update on diagnosis, risk-stratification, and management. Am J Hematol. 2024;99(12):2367–2378.
- Epperla N, Huang Y, Cashen AF, Vaughn JL, Hanel W, Badar T, et al. Evaluation of prognostic factors in patients with high-risk classical Hodgkin lymphoma undergoing autologous transplantation. Blood Adv. 2024;8(21):5458–5466.
- Varma G, Diefenbach C. The role of autologous stem-cell transplantation in classical Hodgkin lymphoma in the modern era. Semin Hematol. 2024;61(4):253–262.
- Luttwak E, Moskowitz AJ. The role of autologous stem-cell transplantation in classical Hodgkin lymphoma in the modern era. Curr Opin Oncol. 2024;35:346–352.
- Abeyakoon C, Kuruvilla J. Optimizing salvage therapy for Hodgkin lymphoma: progress and future challenges. Expert Rev Hematol. 2024;17(8):467–478.
- Savelli CB, Bisio M, Legato L, Fasano F, Santambrogio E, Nicolosi M, et al. Advances in Hodgkin lymphoma treatment: from molecular biology to clinical practice. Cancers (Basel). 2024;16(10):1830.
- Burton C, Allen P, Herrera AF. Paradigm shifts in Hodgkin lymphoma treatment: from frontline therapies to relapsed disease. Am Soc Clin Oncol Educ Book. 2024;44(3):e433502.
- Mariotti J, Ricci F, Giordano L, Taurino D, Sarina B, De Philippis C, et al. Outcome of high-dose chemotherapy followed by autologous stem cell transplantation in relapsed/refractory Hodgkin lymphoma after different numbers of salvage regimens. Cells. 2024;13(2):118.
- Viviani S, Vanazzi A, Frassoni S, Rusconi C, Rossi A, Romano A, et al. High-dose chemotherapy and autologous stem cell transplant as first salvage treatment for relapsed or refractory Hodgkin lymphoma in the era of PET-adapted strategies. Leukemia Lymphoma. 2024;65(4):460–471.
- Zubarovskaya LS, Moiseev IS, Vladovskaya MD, Mikhailova NB, Morozova EV, Bykova TA, et al. Trends in outcome of hematopoietic stem cell transplantation: 5000 transplantations and 30 years of single-center experience. Cancers (Basel). 2023;15(19):4758.
- Randall MP, Spinner MA. Optimizing treatment for relapsed/refractory classic Hodgkin lymphoma in the era of immunotherapy. Cancers (Basel). 2023;15(18):4509.
- Kadkhoda D, Nikoonezhad M, Baghestani AR, Parkhideh S, Momeni-Varposhti Z, Maboudi AAK. Prognostic factors for the long-term survival after hematopoietic stem cell transplantation in patients with Hodgkin lymphoma. Asian Pac J Cancer Prev. 2023;24(2):417–423.
- Armand P, Zinzani PL, Lee HJ, Johnson NA, Brice P, Radford J, et al. Five-year follow-up of KEYNOTE-087:pembrolizumab monotherapy for relapsed/refractory classical Hodgkin lymphoma. Blood. 2023;142(10):878–886.
- Spinner MA, Sica RA, Tamaresis JS, Lu Y, Chang C, Lowsky R, et al. Improved outcomes for relapsed/refractory Hodgkin lymphoma after autologous transplantation in the era of novel agents. Blood. 2023;141(22):2727–2737.
- Gulbrandsen MS, Nøding AS, Smeland KB, Eikeland SA, Kiserud CE, Hjermstad MJ, et al. Health-related quality of life, depressive symptoms, and chronic fatigue in long-term survivors of Hodgkin lymphoma. Leuk Lymphoma. 2023;64(6):1139–1150.
- Josting A, Muller H, Borchmann P, Baars JW, Metzner B, Döhner H, et al. Dose intensity of chemotherapy in patients with relapsed Hodgkin’s lymphoma. J Clin Oncol. 2010;28(34):5074–5080.
- Josting A, Rudolph C, Mapara M, Glossmann JP, Sieniawski M, Sieber M, et al. Cologne high-dose sequential chemotherapy in relapsed and refractory Hodgkin lymphoma: results of a large multicenter study of the German Hodgkin Lymphoma Study Group (GHSG). Ann Oncol. 2005;16(1):116–123.
- Sasse S, Alram M, Müller H, Smardová L, Metzner B, Doehner H, et al. Prognostic relevance of DHAP dose-density in relapsed Hodgkin lymphoma: an analysis of the German Hodgkin-Study Group. Leuk Lymphoma. 2016;57(5):1067–1073.
- Schmitz N, Pfistner B, Sextro M, Sieber M, Carella AM, Haenel M, et al. German Hodgkin’s Lymphoma Study Group; Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. Aggressive conventional chemotherapy compared with high-dose chemotherapy with autologous haemopoietic stem-cell transplantation for relapsed chemosensitive Hodgkin’s disease: a randomised trial. Lancet. 2002;359(9323):2065–2071.
- Stamatoullas A, Brice P, Gueye MS, Mareschal S, Chevallier P, Bouabdallah R, et al. Autologous stem cell transplantation for patients aged 60 years or older with refractory or relapsed classical Hodgkin’s lymphoma: a retrospective analysis from the French Society of Bone Marrow Transplantation and Cell Therapies (SFGM-TC). Bone Marrow Transplant. 2016;51(7):928–932.
- Mounier N, Anthony S, Busson R, Thieblemont C, Ribrag V, Tilly H, et al. Long-term fatigue in survivors of non-Hodgkin lymphoma: the Lymphoma Study Association SIMONAL cross-sectional study. Cancer. 2019;125(13):2291–2299.
- Smeland K, Holte H, Fagerli UM, Bersvendsen H, Hjermstad MJ, Loge JH, et al. Total late effect burden in long-term lymphoma survivors after high-dose therapy with autologous stem-cell transplant and its effect on health-related quality of life. Haematologica. 2022;107(11):2698–2707.
- Georges GE, Bar M, Onstad L, Yi JC, Shadman M, Flowers ME, et al. Survivorship after autologous hematopoietic cell transplantation for lymphoma and multiple myeloma: late effects and quality of life. Biol Blood Marrow Transplant. 2020;26(2):407–412.
- Lemieux C, Ahmad I, Bambace NM, Bernard L, Cohen S, Delisle JS, et al. Evaluation of the impact of autologous hematopoietic stem cell transplantation on the quality of life of older patients with lymphoma. Biol Blood Marrow Transplant. 2020;26(1):157–161.
- Minn AY, Riedel E, Halpern J, Johnston LJ, Horning SJ, Hoppe RT, et al. Long-term outcomes after high dose therapy and autologous haematopoietic cell rescue for refractory/relapsed Hodgkin lymphoma. British J Haematol. 2012;159(3):329–339.
- Ullrich CK, Baker KK, Carpenter PA, Flowers ME, Gooley T, Stevens S, et al. Fatigue in hematopoietic cell transplantation survivors: correlates, care team communication, and patient-identified mitigation strategies. Transplant Cell Ther. 2023;29(3):200.e1–200.e8.
- Metzner B, Müller TH, Casper J, Kimmich C, Petershofen EK, Thole R, et al. Secondary malignancies after autologous stem cell transplantations in patients with malignant lymphoma and multiple myeloma. Eur J Haematol. 2025;114(3):536–544.
- Goodman KA, Riedel E, Serrano V, Gulati S, Moskowitz CH, Yahalom J. Long-term effects of high-dose chemotherapy and radiation for relapsed and refractory Hodgkin’s lymphoma. J Clin Oncol. 2008;26(32):5240–5247.
Keywords
Autologous stem-cell transplantation; Hodgkin lymphoma; Long-term remission; Performance status; Secondary malignancies
Cite this article
Metzner B, Muller TH, Casper C, Kimmich C, Petershofen EK, Thole R, et al. Quality of Long-Term Remissions in Patients with Relapsed Hodgkin Lymphoma after Autologous Stem Cell Transplantation. Clin Oncol J. 2026;7(1):1–6.
Copyright
© 2026 Bernd Metzner. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
