Clinical Image
A 59-year-old man diagnosed with follicular thyroid carcinoma was admitted to our department for ablative Radioiodine Therapy (RAI) following total thyroidectomy. The initial course of RAI was administered with 4.085 MBq of ¹³¹I-NaI under exogenous TSH stimulation. The post-therapy scan revealed focal radioiodine uptake at the right lateral frontal sinus margin. Over the course of three RAIs, totaling 12.739 MBq of ¹³¹I-NaI, the patient achieved complete remission of Differentiated thyroid cancer (DTC), with baseline as well as stimulated thyroglobulin levels remaining below 0.2 ng/ml. Notably, the focal frontal sinus lesion remained unchanged, suggesting a benign nature.
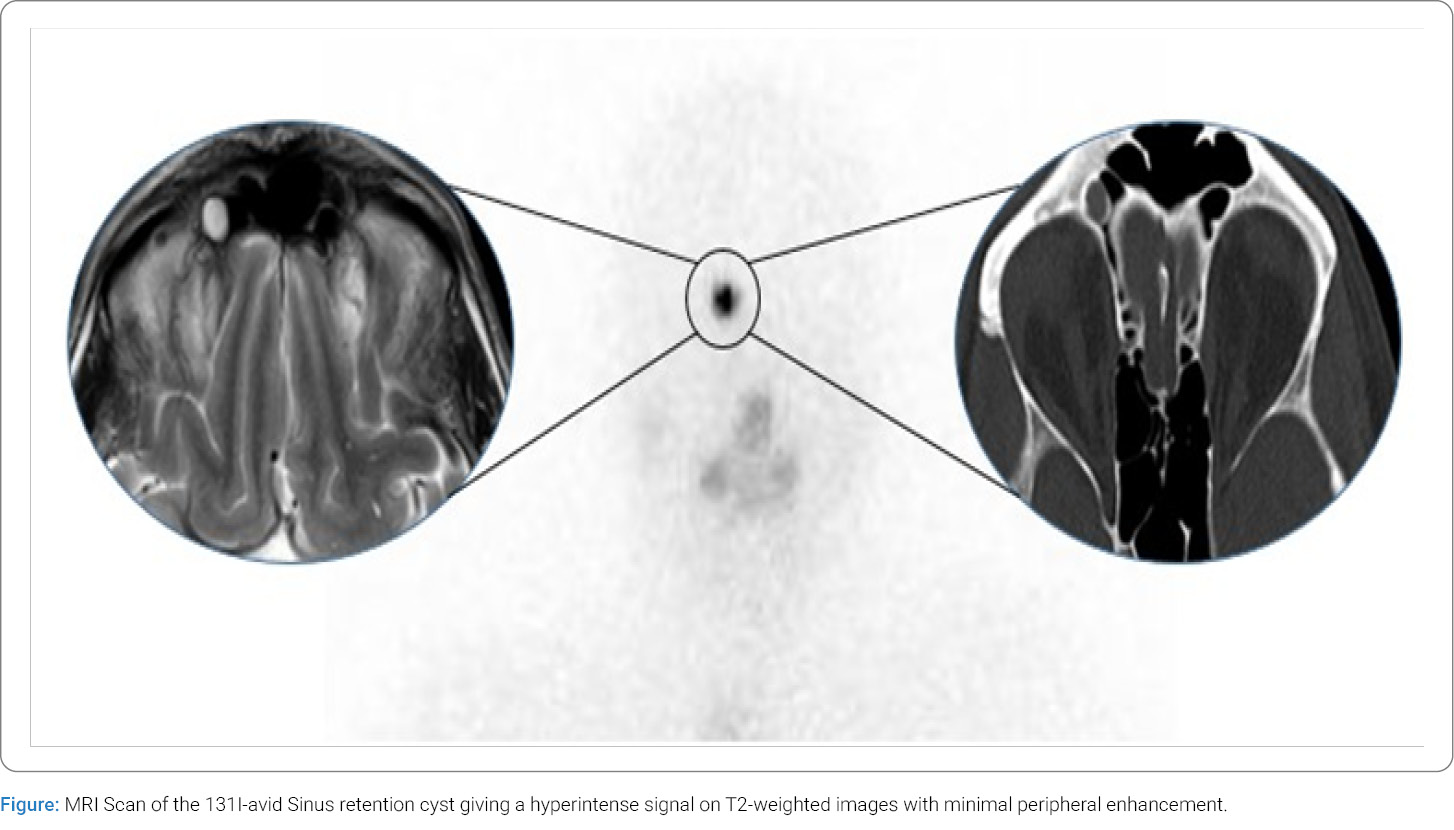
A retrospective assessment of three Computed Tomography (CT) scans performed over three years consistently showed a well-defined, oval-shaped, hypoattenuating lesion (7 mm × 8 mm) at the right lateral frontal sinus margin (right circle). A Magnetic Resonance Imaging (MRI) scan, conducted two years after the initial diagnosis due to sudden hearing loss unrelated to the cancer, confirmed the lesion’s stable size. The MRI also revealed a hyperintense signal on T2-weighted images with minimal peripheral enhancement (left circle).
A relatively common cause of false-positive findings in post-treatment scans is an inflammatory focus, and cases of temporary radioiodine uptake in patients with active sinusitis have been reported [1]. Ciappuccini et al. (2017) published a small case series of iodine-avid mucosal thickening and radioiodine uptake in aspergillomas [2]. However, in our case, the consistent tracer accumulation in ¹³¹I scans, along with the patient’s absence of symptoms, argues against an infectious cause. A mucocele, another differential diagnosis [3], was ruled out, as it would typically show progressive growth over time [4]. Other rarely reported benign lesions with elevated ¹³¹I uptake include cysts, where passive tracer diffusion, or active transport and retention within the cystic cavity are described [1], but none if any cases of iodine-avid sinonasal cysts are formerly reported.
Our case highlights the importance of recognizing cysts as a possible rare benign cause of radioiodine uptake to avoid misdiagnosing them as metastatic disease.
Keywords
Radioiodine; Differentiated thyroid cancer; Sinus retention cyst
Cite this article
Merkle L, Schonemann YI, Vom Scheidt K, Zophel K. A sinus retention cyst mimicking a metastasis of follicular thyroid cancer. Clin Oncol J. 2026;7(1):1–2.
Copyright
© 2026 Merkle L. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
