Abstract
Intussusception is when a proximal segment of the gastrointestinal tract telescopes into an adjacent segment. It is a common presentation in children. On the other hand, intussusception is a rare condition in adults and often points to an underlying pathology. Intussusception in adults should thus raise concerns to the clinician of possible intra-abdominal pathology. In this case, an adult patient presented with recurrent abdominal pain and intestinal obstruction; intussusception was diagnosed on imaging. Surgery and microscopic assessment of resected specimens confirmed a signet-ring cell carcinoma of the colon.
Introduction
Paul Barbette first described intussusception in 1674. Intussusception involves telescoping a bowel segment into an adjacent segment, leading to obstruction, inflammation, and possible ischemia [1]. Although intussusception is the leading cause of intestinal obstruction in children, it is relatively rare after childhood, accounting for less than 5% of bowel obstruction in adults [2]. Four types of intussusception have been described based on the anatomy of the bowel parts involved: (i) ileocolic, which involves the terminal ileum and the ascending colon; (ii) colo-colic, which involves only the colon; (iii) entero-enteric, involves only the small intestine, and (iv) ileocecal, the ileocecal valve forms the lead point of the intussusceptions [3]. In addition, any condition or lesion that affects the normal peristaltic movement of the intestine can precipitate intussusception, with the lesion often serving as the lead point. This case report aims to outline a rare presentation of intussusception in adults.
Case Presentation
A 47-year-old man who presented with a 5-day history of abdominal pain, vomiting, abdominal distension, and constipation. He has had a similar history in the past one year, and this recurs every couple of months. He denies any previous surgeries.
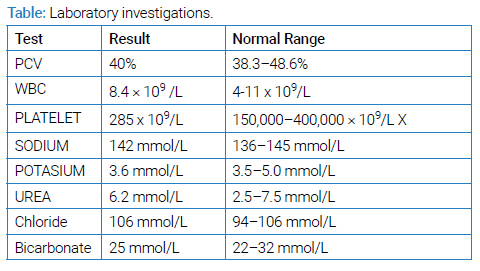
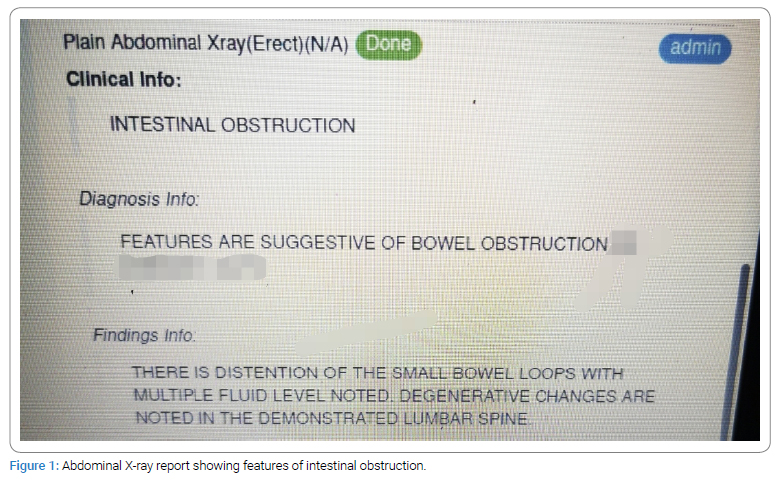
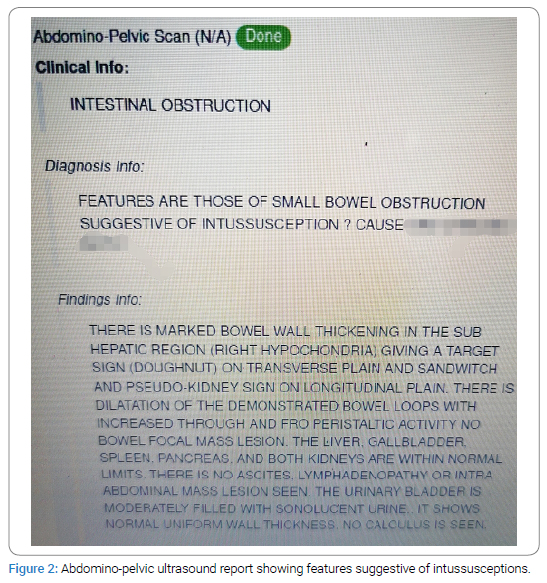
On examination, he was a febrile, and his vitals were normal. He was conscious and alert, fully oriented in person, place, and time. His abdomen was distended, with tenderness around the umbilicus but no rigidity or guarding. He had an ill-defined mass measuring about 2 cm to 3 cm at the epigastric region that extended towards the umbilicus; this was tender, firm, and fixed. Laboratory investigations consisting of Full blood count, Electrolytes, urea, and creatinine are shown in (Table). On this presentation, he had an abdominal X-ray, which showed bowel obstruction features (Figure 1). Next, abdominal ultrasound was done, which showed a target (Doughnut) sign on a transverse plane and a pseudo-kidney sign on the longitudinal plane with moderate ascites. This suggested the presence of an intussusception (Figure 2). This was followed by an abdominal Computed Tomography (CT), which also showed features of intussusception with no signs of ischemia or obstruction (Figure 3).
Following this, an exploratory laparotomy was performed, and an intra-operative finding of intussusception with a colonic bowel tumor around the hepatic flexure (as the lead point for the intussusception) was noted in (Figure 4).

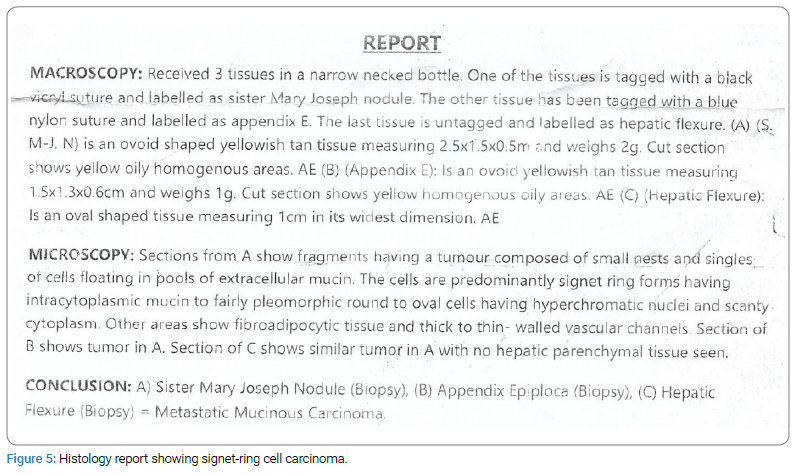
The tumor was resected, and a biopsy was taken from the tumor and sent for histology; histology revealed a signet-ring cell carcinoma of the colon (Figure 5).
The postoperative period was uneventful. He was discharged ten days after the surgery with a plan to commence chemotherapy and regular follow-up.
Discussion
The clinical presentation of adult intussusception is variable, and symptoms are often nonspecific. A study by Carter CR et al. postulates that only about 2–3 cases occur in a population of 1000000 per annum [4]. At the same time, hospital admissions account for less than 0.1 of all adult hospital admissions [5]. Adult intussusception differs from those in children in its cause, presentation, and management. In adults, diagnosis may take a while because of the presentation’s unspecific nature; hence, some patients will only be diagnosed intra-operatively.
Adult intussusception usually has a lead point in the bowel, half of these being malignant lesions [6]. Therefore, the process that leads to intussusception is thought of as a bowel lesion that serves as a lead point and alters the normal peristaltic movement causing an intussusception [7].
The classical presentation in children of colicky pain, bloody mucoid stool, often called ‘currant jelly stool,’ and vomiting is often absent in adults. Instead, a wide array of presentations is often found in adult intussusception and could be chronic or sub-acute. The most common clinical feature of adult intussusception is abdominal pain [8]. Along with abdominal pain, there are often nonspecific signs of bowel obstruction, like constipation, nausea, vomiting, and gastrointestinal bleeding [9]. Diagnosis of intussusception in Adults is often radiological due to the vague presentation. CT scan is the investigation of choice with a diagnostic accuracy of 58% to 100% and a specificity of 57% to 71% [8]. The CT shows a mass-like lesion that appears as a “target” or a “sausage” mass [8]. Oftentimes, especially in resource-constrained settings, ultrasonography is often used to evaluate intussusception with the classic features, including the “target and doughnut sign” in transverse view and the “pseudo kidney sign” in longitudinal view [10].
The preoperative diagnostic accuracy of ultrasonography is 78.5%. In cases of palpable abdominal mass, the diagnostic accuracy of ultrasonography is even better at 86.6% [11].
There is no formal universal approach to managing intussusception. However, operative management is usually suggested due to the underlying pathology causing intussusception in adults and the suspicion of a tumor serving as the lead point [12]. In addition, treatment may include other adjuncts like chemotherapy and radiotherapy, depending on the underlying cause of the intussusception and the operative findings.
In conclusion, intussusception is a common complication of colonic tumors. This case report demonstrated a signet-ring cell carcinoma of the colon, which caused an intussusception, as shown by US and CT. Signet-ring cell carcinoma is a malignant tumor in which a definitive diagnosis can be made by histology. This tumor can precipitate an intussusception and clinical intestinal obstruction; hence, a combination of bowel resection and adjunctive therapy may be required to manage this distinctive type of presentation.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
Keywords
Intussusception; Adults; Signet-ring; Colon
Cite this article
Abu MF. A rare case of recurrent intussusception in an adult secondary to signet-ring cell carcinoma of the colon. Clin Oncol J. 2023;4(1):1–5.
Copyright
© 2023 Moses F Abu. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
